
Conveying unfavorable medical news is a critical component of patient and familial care, presenting an enduring challenge for health-care professionals. Such news refers to information that profoundly and detrimentally influences an individual's perception of their future[1] and has implications for the patient, family members, and the health professional. Effectively managing the communication of bad news requires a wide range of professional competencies that incorporate attitudes, knowledge, and skills. The health-care provider must be able to discern and respond to patients’ emotions demonstrating empathy[2].
For the physician, communicating unpleasant news can negatively affect job satisfaction, leading to compassion fatigue and burnout[3,4]. Given the severity of these effects, medical institutions have deemed it necessary to allocate educational resources toward equipping medical students with this vital capability during their academic years, fostering its development throughout their medical careers.
The methodology of this systematic review complies with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 checklist. The Medline – PubMed and Scopus bibliographic databases were searched from 1 to 4 of February 2023 using the following keywords: medical education, breaking bad news, and end of life communication.
We included studies that met the following inclusion criteria:
- -
articles written in English and
- -
no restrictions were placed on the study design and fieldwork settings.
We searched three electronic databases (platform in brackets):
- -
Medical Literature Analysis and Retrieval System Online [MEDLINE] (OVID)
- -
Scopus
Following the PRISMA guidelines[5], two different electronic databases (PubMed and Scopus) were searched from February 1 to 4 to locate potentially relevant articles. We used the search terms medical education, breaking bad news, and end of life communication. We searched for the Medical Subject Headings (MesH) and free-text phrases such as synonyms or abbreviations.
The following data were extracted from each included study: author, year of publication, digital object identifier, country and setting of the study, study aim, study design and data collection method, and summary of key study findings.
The systematic search strategy identified 503 potentially relevant articles, of which six were removed as duplicates. Of the remaining 497 articles, 429 did not meet the eligibility criteria and were therefore excluded from this review. Following screening and detailed assessment of the full text, a further 47 articles were excluded for various reasons (training programs, breaking bad news [BBN] of coronavirus disease 2019 [COVID-19] or injury, editorial letter), resulting in 21 studies being deemed appropriate for inclusion in this systematic review (Figure 1).
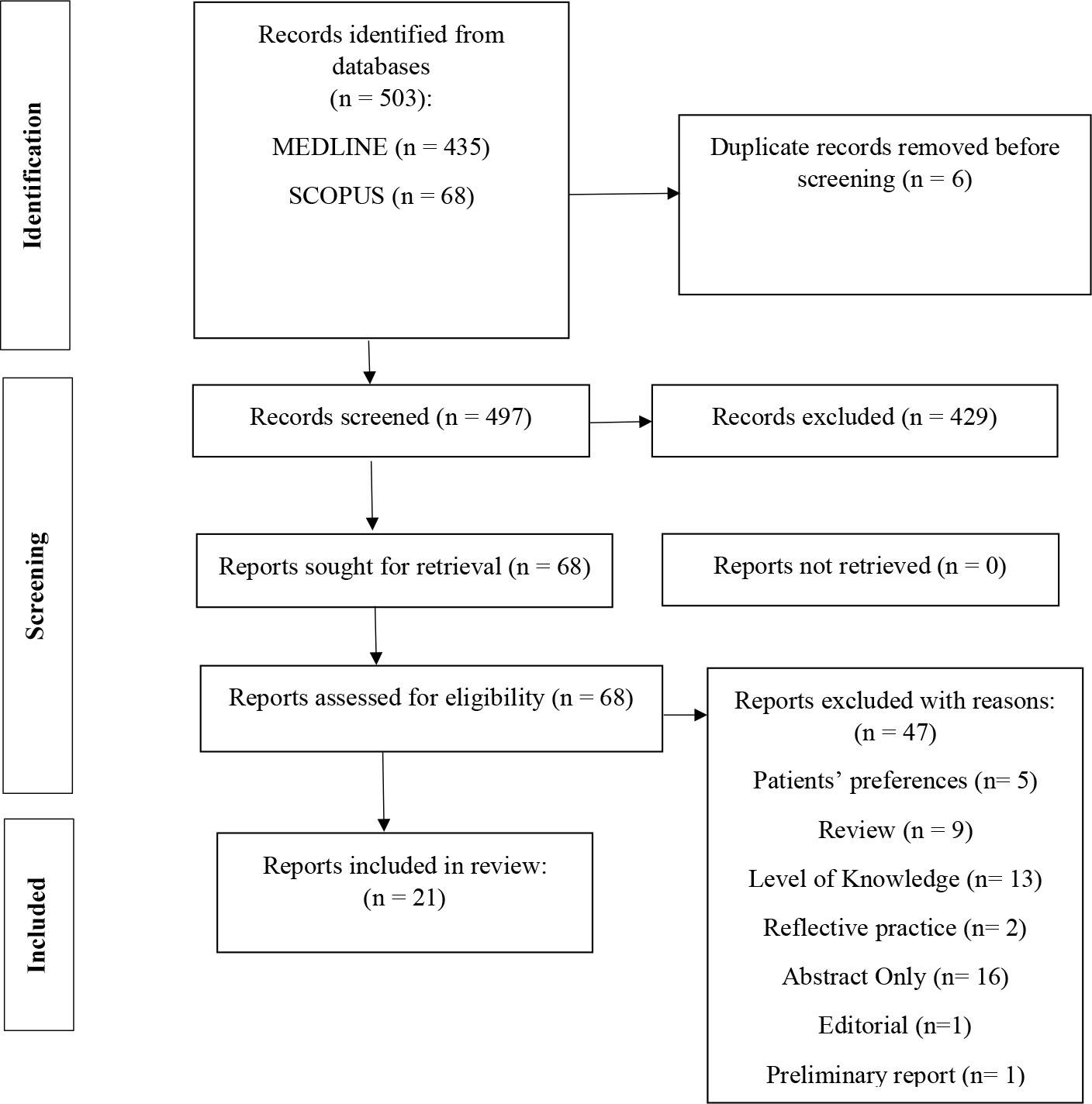
PRISMA flow diagram.
A review of the available literature resulted in selection of 21 publications to be included in this study. Of these 21 articles, 19 referred to the assessment of training courses, training programs, and simulation-based workshops for medical students and residents regarding BBN, one focused on videotaped consultations, while the remaining one referred to the assessment of a theater course (Table 1).
Summary of the studies included in this systematic review.
| Author(s), Year | Digital Object Identififier (DOI) | Country | Setting | Study Aim | Data Collection Method and Study Design | Summary of Key Study Findings |
|---|---|---|---|---|---|---|
| Bishop et al.(2016) | http://dx.doi.org/10.1177/0091217416659272 | USA | East Tennessee State University (ETSU) Graduate Storytelling Program and the departments of Family and Internal Medicine at the James H. Quillen College of Medicine. | To assist learners in: (1) understanding a five-step patient-centered model that is based upon needs, preferences, and expectations of patients with cancer and (2) individualizing communication that is consistent with patient preferences in discussing emotions, informational detail, prognosis and timeline, and whether or not to discuss end-of-life issues | A randomized control study. A patient-centered web-based/digital Breaking Bad News communication training module designed to educate learners of various levels and disciplines was used based upon video-recorded patient stories. | Medical students and resident physicians improved their communication skills with the Breaking Bad News module. |
| Bonnaud,- Antignac et al. (2009) | https://doi.org/10.1002/pon.1649 | France | University of Nantes | To assess the performance of the training course on the disclosure of a diagnosis of cancer intended for fifth year medical students of the University of Nantes | The course comprised three sessions: (1) a group discussion that taught a six-point protocol (SPIKES) for delivering a diagnosis, (2) a videotaped simulated interview to assess protocol implementation and communication skills, and (3) feedback from a senior physician. The learning objectives were memorisation and implementation of the protocol, use of appropriate communication techniques to deal with the patient's response, and identifying one's own reactions in a stressful situation. Two types of assessments were performed before and after each session: self-assessments by the students and a quantitative and qualitative external assessment by a psychologist and senior physician. In addition, recall of the six-point protocol was assessed during the end-of-the-year examination. | Our training course on communication techniques helps students acquire confidence in their skills in breaking bad news by backing theory with practice and feedback. The students make progress despite the psychological stress generated by simulated real-life conditions. |
| Cannone et al. (2019) | https://doi.org/10.15766/mep_2374-8265.10819 | USA | University of Tennessee Health Science Center. | To improve communication skills in trainees by providing a safe environment to learn and practice. | An eight-module course on communication in oncology practice was delivered over 2 months for palliative and oncology fellows and radiation oncology residents. | Twenty-two learners participated over 2 years of this course. Participants reported a significant increase in perceived competence in all areas on the postcourse survey. SP feedback on OSCEs pre- and post-course indicated improvement in skills for learners. Pre- and post-course OSCE video assessment revealed a significant improvement in global communication skills. |
| Curtis et al. (2013) | https://doi.org/10.1001/jama.2013.282081 | USA | University of Washington and Medical University of South Carolina. | To assess the effects of a communication skills intervention for internal medicine and nurse practitioner trainees on patient- and family-reported outcomes. | A randomized trial. 91 internal medicine and 81 nurse practitioner trainees were randomized to an 8-session, simulation-based, communication skills intervention (N = 232) or usual education (N = 240). | Simulation-based communication training compared with usual education did not improve quality of communication about end-of-life care or quality of end-of-life care but was associated with a small increase in patients’ depressive symptoms. |
| Curtis et al. (2018) | https://doi.org/10.1001/jamainternmed.2018.2317 | USA | Clinicians were recruited from 2 large health care systems in the Pacific Northwest. One includes 2 academic and 2 community hospitals, a comprehensive cancer center, and an extensive outpatient network; the other includes 3 community hospitals and an extensive outpatient network. | To evaluate the efficacy of a patient-specific preconversation communication-priming intervention (Jumpstart-Tips) targeting both patients and clinicians and designed to increase goals-of-care conversations compared with usual care. | A randomized clinical trial. Clinicians were randomized to the bilateral, preconversation, communication-priming intervention (n = 65) or usual care (n = 67), with 249 patients assigned to the intervention and 288 to usual care. | This intervention increased the occurrence, documentation, and quality of goals-of-care communication during routine outpatient visits and increased goal-concordant care at 3 months among patients with stable goals, with no change in symptoms of anxiety or depression. |
| Day et al. (2015) | https://doi.org/10.1097/ACM.0000000000000607 | USA | University of California, Davis School of Medicine (UC Davis). | To examine the impact on medical student outcomes of medical content taught via an eLearning format in comparison with a well-established small-group format at one institution. | A quasi-randomized educational study of third-year medical students. ll 119 third-year medical students at UC Davis participated in the yearlong Doctoring III PEOL course (Doctoring). A subset of students was randomized to additionally participate in eDoctoring. | Findings showed equivalent gains in self-efficacy and knowledge between students participating in a Web-based PEOL curriculum in comparison with students learning similar content in a small-group format. |
| Epstein et al. (2017) | https://doi.org/10.1001/jamaoncol.2016.4373 | USA | Community- and hospital-based cancer clinics in Western New York and Northern California; | To determine whether a combined intervention involving oncologists, patients with advanced cancer, and caregivers would promote patient-centered communication, and to estimate intervention effects on shared understanding, patient-physician relationships, QOL, and aggressive treatments in the last 30 days of life. | A cluster RCT. Oncologists received individualized communication training using standardized patient instructors while patients received question prompt lists and individualized communication coaching to identify issues to address during an upcoming oncologist visit. | A combined intervention that included oncologist communication training and coaching for patients with advanced cancer was effective in improving patient-centered communication but did not affect secondary outcomes. |
| Gorniewicz et al. (2017) | https://doi.org/10.1016/j.pec.2016.11.008 | USA | The East Tennessee State University (ETSU) Graduate Storytelling Program and the departments of Family and Internal Medicine. | To test the effectiveness of a brief, self-paced, skill-focused BBN training module using objective evaluation measures. | This randomized control study (N = 66) compared intervention and control groups of students (n = 28) and residents’ (n = 38) objective structured clinical examination (OSCE) performance of communication skills using Common Ground Assessment and Breaking Bad News measures. | This brief BBN training module is an effective method of improving BBN communication skills among medical students and residents. |
| Harnischfeger et al. (2022) | https://doi.org/10.1016/j.esmoop.2022.100623 | Germany | Five University Medical Centers i | To investigate the effect of a newly developed compact communication skills training ‘PAL-LI-COM’ on oncologists’ competencies to early address PC/EoL-related issues. | A randomized, controlled trial (RCT) with an intervention group (IG; 2 × 90 min training) and a wait list control group (CG) at five sites. At two assessment points, participating oncologists led videotaped medical consultations with simulated patients (SPs) via a privacy compliant video conference platform. SPs were represented by trained actors. | Findings indicate that the compact communication skills training PALLI-COM increases oncologists’ competencies in early addressing PC/EoL-related issues from different perspectives. Implementation in routine oncology residency might improve advanced cancer care by strengthening these communication skills. |
| Henselmans et al. (2019) | https://doi.org/10.1634/theoncologist.2019-0453 | Netherlands | Academic Medical Center, University of Amsterdam | To examine the independent and combined effect of an oncologist training and a patient communication aid on SDM. | A multicenter randomized controlled trial with four parallel arms (2016–2018), oncologists (n = 31) were randomized to receive SDM communication skills training or not. The training consisted of a reader, two group sessions, a booster session, and a consultation room tool (10 hours). Patients (n = 194) with advanced cancer were randomized to receive a patient communication aid or not. The aid consisted of education on SDM, a question prompt list, and a value clarification exercise. | The oncologist training had a large positive effect on observed SDM (Cohen's d = 1.12) and on patient reported SDM (d = 0.73). The patient communication aid did not improve SDM. The combination of interventions did not add to the effect of training oncologists only. The interventions affected neither patient nor oncologist satisfaction with the consultation nor patients’ decisional conflict, quality of life, consultation duration, or the decision made. |
| Kron et al. (2017) | https://doi.org/10.1016/j.pec.2016.10.024 | USA | Three US medical schools: Eastern Virginia Medical School (EVMS); the University of Michigan Medical School (UM); and the University of Virginia School of Medicine (UVA). | To assess advanced communication skills among second-year medical students exposed either to a computer simulation (MPathic-VR) featuring virtual humans, or to a multimedia computer-based learning module, and to understand each group's experiences and learning preferences. | A single-blinded, mixed methods, randomized, multisite trial compared MPathic-VR (N = 210) to computer-based learning (N = 211). | MPathic-VR was effective in training advanced communication skills and in enabling knowledge transfer into a more realistic clinical situation. |
| Lienard et al. (2010) | https://doi.org/10.1038/sj.bjc.6605749 | Belgium | A University medical hospital. | To assess the efficacy of a 40-h training programme designed to teach residents the communication skills needed to break the bad news. | A randomised study. Residents were randomly assigned to the training programme or to a waiting list. A simulated patient breaking bad news (BBN) consultation was audiotaped at baseline and after training in the training group and 8 months after baseline in the waiting-list group. Transcripts were analysed by tagging the used communication skills with a content analysis software (LaComm) and by tagging the phases of bad news delivery: pre-delivery, delivery and post-delivery. Training effects were tested with generalised estimating equation (GEE) and multivariate analysis of variance (MANOVA). | The trained residents (n=50) used effective communication skills more often than the untrained residents (n=48): more open questions (relative rate (RR)=5.79; P<0.001), open directive questions (RR=1.71; P=0.003) and empathy (RR=4.50; P=0.017) and less information transmission (RR=0.72; P=0.001). The pre-delivery phase was longer for the trained (1 min 53 s at baseline and 3 min 55 s after training) compared with the untrained residents (2 min 7 s at baseline and 1 min 46 s at second assessment time; P<0.001). |
| Merchaert et al. (2013) | https://doi.org/10.1038/bjc.2013.615 | France | Hospital | To evaluate if the BIC-CST programme will lead to n improvement in the time allocated to each of the three phases of the BBN process, including a longer pre-delivery phase and a shorter delivery phase, in a simulated BBN triadic consultation. The second hypothesis is that residents will include the simulated relative sooner over the course of the consultation and will generally promote his or her participation, especially response to the bad news, following training. Third, trained residents will have acquired assessment and supportive skills that will help them to be more focused on both the simulated patient and the simulated relative during a BBN consultation. As a result, the simulated patient and simulated relative would be expected to more readily express their concerns. | Residents were randomly assigned to a 40-h dyadic and triadic communication skills training programme (n=48) or a waiting list (n=47). A simulated BBN triadic consultation was audiotaped at baseline, and after training for the training group, and 8 months after baseline for the waiting list group. Transcripts were analysed using content analysis software (LaComm). A coder determined the moment of bad news delivery and the relative's first turn of speech regarding the bad news. A generalised estimating equation was used to evaluate residents’ communication skills, BBN timing, and the relative's inclusion in the consultation. | A training program that focuses on the practice of dyadic and triadic communication skills can improve the communication skills of the participating residents in a BBN triadic consultation. |
| Meunier et al. (2013) | https://doi.org/10.1016/j.pec.2013.04.020 | Belgium | Hospitals. | To assess training effect on residents’ physiological arousal. | Residents’ physiological arousal was measured, in a randomized controlled trial design, by heart rate and salivary cortisol before, during and after a BBN simulated task. | Communication skills training has an effect on residents’ physiological arousal. Residents’ self-efficacy and communication skills improvements in a BBN simulated task are associated with an elevated physiological arousal, which becomes proportional to the complexity of the task and reflects a better engagement and performance. |
| Shildmann et al. (2011) | https://doi.org/10.1055/s-0031-1275802 | Germany | 4 hospitals | To evaluate the concept of an obligatory postgraduate course for physicians on breaking bad news. | An interventional study without control group was carried out in which a questionnaire (closed-ended questions and Likert scales as well as open-ended questions) was distributed before and immediately after the course. 186 physicians participated in the study. | Compared with the beginning of the course the respondents rated their communication skills significantly better at the end of the course. The course's relevance for clinical practice, teaching methods and the organisation of the course were rated positively. |
| Servotte et al. (2019) | https://doi.org/10.5811/westjem.2019.8.43441 | Belgium | Emergency Department (ED) | To assess the efficacy of a four-hour BBN simulation-based training on perceived self-efficacy, the BBN process, and communication skills. | Medical students and residents were randomized into a 160-hour ED clinical rotation without a formal BBN curriculum (control group [CG], n = 31) or a 156-hour ED clinical rotation and a four-hour BBN simulation-based training (training group [TG], n = 37). Both groups were assessed twice: once at the beginning of the rotation (pre-test) and again four weeks later. Assessments included a BBN evaluation via a simulation with two actors playing family members and the completion of a questionnaire on self-efficacy. Two blinded raters assessed the BBN process with the SPIKES (a delivery protocol for delivering bad news) competence form and communication skills with the modified BBN Assessment Schedule. | A short BBN simulation-based training can be added to standard clinical rotations. It has the potential to significantly improve self-efficacy, the BBN process, and communication skills. |
| Setubal et al. (2017) | https://doi.org/10.1055/s-0037-1604490 | Brazil | Hospital | To analyze the perception of residents regarding a training program in communicating bad news in perinatology based on video reviews and setting, perception, invitation, knowledge, emotion, and summary (SPIKES) strategy. | A randomized controlled intervention study to evaluate the efficacy of a training program on improving residents’ skills to communicate bad news. Data were collected using a Likert scale. | The majority of the residents evaluated training highly as an education activity to help increase knowledge, ability and understanding about breaking bad news in perinatology. |
| Setubal et al. (2018) | https://doi.org/10.1055/s-0037-1621741 | Brazil | Medical school. | To evaluate whether a structured training session would enhance perinatology residents’ skills in BBN. | A randomized controlled intervention study with year 1 to 4 Perinatology residents from a medical school in Brazil, during the 2014/15 school year. A total of 61 out of 100 (61%) eligible residents volunteered to a structured training program involving communicating a perinatal loss to a simulated patient (SP) portraying the mother followed by the SP's immediate feedback, both video recorded. | The SPIKES training did not significantly impact the residents’ performance. The residents endorsed the simulation with feedback as a useful training modality. Further research is needed to determine which modality is more effective. |
| Skye et al. (2014) | https://doi.org/10.1007/s13187-014-0641-y | USA | University | To explore the contexts, approaches, experiences, and reactions in giving and receiving bad news | Second-year medical students participated in a required educational session that utilized interactive theater which helps students learn about the issues of breaking bad news to a patient with cancer. Following the interactive theater piece, professional actors provided students role play experiences in small groups with breaking bad news. Anonymous evaluation surveys were given out to all second-year medical students at the conclusion of the breaking bad news session. Surveys contained quantitative and qualitative responses. Three years of evaluations were analyzed. A total of 451 (88 %) students completed the evaluations | This type of interactive theater, combined with role play exercises with professional actors, is extremely well received and enhances students’ understanding with the challenges of, and approaches to, breaking bad news. |
| Tobler et al. (2014) | https://doi.org/10.1097/SIH.0000000000000031 | USA | University of Calgary | To develop and evaluate the effectiveness of a simulation-based workshop for teaching pediatric trainees’ communication skills in breaking bad news. | A simulation-based workshop was developed to teach skills in breaking bad news. After a classroom-based introduction, small groups of residents participated in 3 scenarios, each starting with a simulated resuscitation, followed by 2 conversations with the patient's parent, played by actors. Each conversation was observed through a 1-way mirror and was followed by a debriefing. After the workshop, the residents completed workshop evaluations and a self-assessment. | Residents’ ratings of the workshop were very high for all items, and 100% of the residents reported improvement in their ability to deliver bad news after the workshop. Statistically significant improvement was found in 14 of 17 items of the evaluation tool used by experts and parents, with the parents reporting greater improvement than the experts. |
| Watling & Brown (2007) | https://doi.org/10.1212/01.wnl.0000280461.96059.44 | USA | University of Western Ontario | To develop a communication skills training program specifically for neurology residents, directed at some of the most challenging clinical scenarios that they will face in practice, and to foster reflective practice as a tool for enhancement of communication skills. | A group of 12 neurology residents participated in a series of six case-based communication skills workshops. Each workshop focused on a particular clinical scenario, including breaking bad news, discussing do-not-resuscitate orders, communicating with “difficult” patients, disclosing medical errors, obtaining informed consent for neurologic tests and procedures, and discussing life-and-death decisions with families of critically ill patients. Residents also kept reflective portfolios in which real examples of these interactions were recorded. | The program was well accepted, and residents rated the workshops as effective and relevant to their practice. |
Bishop et al.[6] conducted a workshop that showcased the effectiveness of a patient-centered, web-based/digital training module for conveying bad news. This module was designed to cater to learners across various levels and disciplines.
The study by Bonnaud-Antignac et al.[7] assessed the performance of a training course, which was intended for fifth-year medical students, on the disclosure of a diagnosis of cancer. The course comprised three sessions: a group discussion that taught a six-point protocol (setting, perception, invitation, knowledge, emotion, and summary [SPIKES]) for delivering a diagnosis, a videotaped simulated interview to assess protocol implementation and communication skills, and feedback from a senior physician. The results demonstrated that the training course that was used helped students to acquire confidence in their skills in BBN by backing theory with practice and feedback.
Cannone et al.[8] implemented an eight-module course on communication in oncology practice over 2 months for palliative and oncology fellows and radiation oncology residents. According to the results, all the participants reported a significant increase in perceived competence in all areas on the post-course survey.
Moreover, the study by Curtis et al.[9] assessed the effects of a communication skills intervention for internal medicine and nurse practitioner trainees on patient- and family-reported outcomes. Participants were randomized to an eight-session, simulation-based, communication skills intervention or usual education. The study concluded that simulation-based communication training did not improve the quality of communication about end-of-life care or the quality of end-of-life care itself. However, it was associated with a small increase in patients’ depressive symptoms.
The study by Day et al.[10] compared the effect of web-based eLearning versus small-group learning on medical student outcomes. Students were randomly assigned to web-based eDoctoring (n = 48) or small-group doctoring (n = 71) curriculum. Findings showed equivalent gains in self-efficacy and knowledge between students participating in a web-based PEOL curriculum in comparison to students learning similar content in a small-group format.
Epstein et al.[11] examined whether a combined intervention involving oncologists, patients with advanced cancer, and caregivers would promote patient-centered communication and estimated the effects of intervention on shared understanding, patient–physician relationships, quality of life (QOL), and aggressive treatments in the last 30 days of life. Oncologists received individualized communication training from standardized patient instructors, while patients received question prompt lists and individualized communication coaching to identify the issues to address during an upcoming oncologist visit. Overall, a combined intervention that included oncologist communication training and coaching for patients with advanced cancer was effective in improving patient-centered communication, but did not affect secondary outcomes.
The study by Gorniewicz et al.[12] tested the effectiveness of a brief, learner-centered BBN communication skills training module using objective evaluation measures. This randomized controlled study (N = 66) compared intervention and control groups of students’ (n = 28) and residents’ (n = 38) objective structured clinical examination (OSCE) performance of communication skills using Common Ground Assessment and BBN measures. Results indicated that this brief BBN training module is an effective method of improving BBN communication skills among medical students and residents.
Harnischfeger et al.[13] investigated the effect of a newly developed compact communication skills training “PALLI-COM” on oncologists’ competencies to address PC/EoL-related issues early. A randomized controlled trial with an intervention group and a waitlist control group at five sites was conducted. At two assessment points, participating oncologists led videotaped medical consultations with simulated patients (SPs) via a privacy compliant video conference platform. SPs were represented by trained actors. Findings indicated that the compact communication skills training PALLI-COM increases oncologists’ competencies in addressing PC/EoL-related issues early from different perspectives, thus improving advanced cancer care.
The study by Henselmans et al.[14] conducted in the Netherlands examined the independent and combined effect of an oncologist training and a patient communication aid on SDM. According to the results, training medical oncologists in SDM about palliative systemic treatment improves both observed and patient-reported SDM.
Kron et al.[15] assessed advanced communication skills among second-year medical students exposed either to a computer simulation (MPathic-VR) featuring virtual humans or to a multimedia computer-based learning module. MPathic-VR–trained students improved their intercultural and interprofessional communication performance between their first and second interactions with each scenario.
The study by Lienard et al.[16] assessed the efficacy of a 40-h training program designed to teach residents the communication skills needed to break the bad news. An SP BBN consultation was audiotaped at baseline and after training in the training group and 8 months after baseline in the waiting list group. The trained residents used effective communication skills more often than the untrained residents, thus indicating that the way residents break bad news may be improved.
Merchaert et al.[17] examined the efficacy of training programs designed to teach residents the communication skills needed to break bad news in a triadic consultation. The results indicated that a training program that focuses on the practice of dyadic and triadic communication skills can improve the communication skills of the participating residents in a BBN triadic consultation.
The study by Meunier et al.[18] assessed the effect of a communication skills training on residents’ physiological arousal during a BBN task. Findings demonstrated that the residents’ self-efficacy and communication skills improvements in a BBN simulated task are associated with an elevated physiological arousal.
Shildmann et al.[19] assessed the results of an obligatory postgraduate course for physicians on BBN. One hundred and eighty-six physicians in a German hospital participated in the study. One hundred and two respondents (54.8 %) had broken bad news more than five times per month. Seventy-five physicians (40.3 %) indicated that they had never participated in a teaching module on this topic before the course. The respondents rated their communication skills significantly better at the end of the course compared to the beginning of the course.
Servotte et al.[20] conducted a randomized controlled study that was aimed to assess the efficacy of a 4-h BBN simulation-based training on perceived self-efficacy, the BBN process, and communication skills. In this study, medical students and residents were randomized into a 160-h ED clinical rotation without a formal BBN curriculum (control group [CG], n = 31) or a 156-h ED clinical rotation and a 4-h BBN simulation-based training (training group [TG], n = 37). Both groups were assessed twice: once at the beginning of the rotation (pre-test) and again 4 weeks later. Assessments included a BBN evaluation via a simulation with two actors playing family members and the completion of a questionnaire on self-efficacy. Two blinded raters assessed the BBN process with the SPIKES (a delivery protocol for delivering bad news) competence form and communication skills with the modified BBN Assessment Schedule. The results revealed that after the training, students with limited clinical experience before the rotation showed BBN performance skills equal to those of students in the CG who had greater clinical experience.
The study by Setubal et al.[21] analyzed the perception of residents regarding a training program in communicating bad news in perinatology based on video reviews and SPIKES strategy. An analysis of complementary data collected from participants in a randomized controlled intervention study was performed to evaluate the efficacy of a training program on improving residents’ skills to communicate bad news. Half of the group received training, consisting of discussions of video reviews of participants’ simulated encounters communicating a perinatal loss to a “mother” based on the SPIKES strategy. Residents took SPIKES training as a guide to systematize the communication of bad news and to amplify perceptions of the emotional needs of the patients. They suggested the inclusion of a similar training in their residency programs curricula.
Another study by Setubal et al.[22] evaluated whether a structured training session would enhance perinatology residents’ skills in BBN. A randomized controlled intervention study with year 1–4 perinatology residents from a medical school in Brazil was conducted. The simulations used lasted on average 12 min, feedback was for 5 min, and SPIKES training was between 1 h and 2 h 30 min. There was no significant difference in the residents’ performances according to the SPs’ evaluations; therefore, further research is needed to determine which modality is more effective.
The study by Skye et al.[23] investigated the use of interactive theater and role play with professional actors in teaching BBN to medical students. Second-year medical students participated, and professional actors provided students role play experiences in small groups with BBN. According to the results, interactive theater, combined with role play exercises with professional actors, is extremely well received and enhances students’ skills on communicating bad news.
Tobler et al.[24] evaluated the effectiveness of a simulation-based workshop for teaching pediatric trainees’ communication skills in BBN and found that this workshop successfully improved pediatric trainees’ skills in having difficult conversations with families.
Finally, the study by Watling & Brown[25] aimed to enhance learning of these skills and to encourage reflective practice around communication skills. A group of 12 neurology residents participated in a series of six case-based communication skills workshops. Each workshop focused on a particular clinical scenario and the results indicated that the use of portfolios may promote lifelong learning in this area.
A search of the literature led to the identification of studies that involved different teaching strategies for medical students, residents, and experienced physicians. It appeared that medical residents are the most commonly studied group, which is likely due to their transition toward actual medical practice.
In terms of teaching techniques of communicating bad news, the most effective methods seem to be the adoption of mixed strategies because it involves different types of approaches. However, a direct comparison between different methods cannot conclusively establish the most effective technique. This may be due to the fact that the best method of training depends on the medical curriculum of each country and also on the structure of the health-care system in each country.
Limitations were present in the reviewed studies, including small sample sizes, lack of control groups, and absence of long-term follow-up. These limitations hinder comprehensive understanding and comparison of the effectiveness of the teaching techniques.
In addition, although the studies reported the methods for each approach, the details were not fully described. This, along with the challenges of assessing students with a standardized checklist, made it difficult to determine the best method of teaching communicating bad news.
Another limitation is that two of the studies were conducted in Brazil, two in France, three in Belgium, two in Germany, and one in the Netherlands, while most of the studies, 10 in number, were conducted in the USA. The fact that most studies were conducted in a single geographic area is a limitation, as factors such as social and cultural context influence aspects of the topic under investigation.
Finally, it should be noted that although in all studies, the implementation of a teaching program had positive effects on the development of students’ and physicians’ skills of communicating bad news, the effectiveness of each protocol in a large sample size should be investigated, providing future feedback to conduct comparable and valid results.
The results of this systematic review suggest that a range of methods can be effective in teaching medical students and residents how to communicate bad news. Mixed methods, such as training programs combined with videotaped simulations, demonstrated particularly encouraging results. Nevertheless, all investigated techniques had a positive impact on medical education concerning the communication of bad news.
Despite inherent limitations in the studies, the results support the importance of communicating bad news in medical education. Therefore, it is deemed necessary to integrate BBN education into the curriculum of medical schools and continuing medical education.
Doing so can help ensure that future doctors are equipped with the necessary communication skills to handle these difficult conversations sensitively and effectively. This not only enhances patient care, but also contributes to better patient–doctor relationships and may aid in mitigating potential emotional distress caused by poor communication of negative medical news.