
Health is a multidimensional construct shaped by the interaction of physical, mental, and social factors. Adequate levels of daily physical activity (PA) are among the most important determinants of health across the lifespan and contribute to the prevention of numerous chronic diseases (Chen et al., 2023). This issue is particularly relevant during childhood (0–9 years) and adolescence (10–19 years), a critical developmental period for establishing lifelong health-related behaviors (World Health Organization, 2025).
Regular PA has well-documented benefits for physical and mental health, including improvements in body composition, cardiovascular and metabolic function, blood pressure regulation, and psychological well-being (Herbert, 2022). Even modest increases in PA are associated with a reduced risk of chronic disease and premature mortality (Warburton et al., 2006).
In children and adolescents, insufficient PA and sedentary lifestyles are strongly linked to overweight and obesity, which often persist into adulthood and negatively affect long-term quality of life (Gavela-Pérez et al., 2023; Nagata et al., 2023b). In response, the World Health Organization (WHO) recommends that children and adolescents aged 5–17 years engage in at least an average of 60 min per day of moderate- to vigorous-intensity physical activity (MVPA) to obtain health benefits (World Health Organization, 2020).
One of the main barriers to achieving recommended PA levels among adolescents is excessive screen time. High engagement in screen-time-based behaviors is consistently associated with lower PA, increased adiposity, and adverse behavioral and mental health outcomes (Nagata et al., 2023a; Serrano-Sanchez et al., 2011). Moreover, prolonged screen time has been associated with disruptions in social relationships and reduced opportunities for face-to-face interaction, which can negatively influence adolescents’ engagement in PA, as demonstrated in epidemiological studies (Alotaibi et al., 2020; American Academy of Pediatrics, 2025; Zablotsky et al., 2025).
Recent evidence supports that these risk factors commonly co-occur and interact to influence PA and weight outcomes. Haghjoo et al. (2022) reported a positive association between higher screen time and adolescent overweight/obesity, and Nagata et al. (2023b) found that high screen time combined with low PA was strongly associated with higher overweight and obesity risk (Nagata et al., 2023b). Lin et al. (2024) reported a moderate positive association between social support and adolescent PA, with self-efficacy acting as a key mediator. Other studies indicate that combined approaches (PA together with behavioral and psychosocial support) are more effective than single-focus strategies for improving activity and related outcomes (Qiu et al., 2022; Zhou et al., 2025). Taken together, these findings reinforce the need for an integrated perspective when developing PA recommendations for adolescents (van Sluijs et al., 2021).
Importantly, the relationship between screen time, PA, and health outcomes is complex and may depend on the type of screen activity and the behaviors it replaces, as well as individual and social factors (Zink et al., 2024). Participation in organized PA reduces some negative effects of excessive screen time, highlighting the importance of supportive environments that encourage active lifestyles (Maitland et al., 2013; Serrano-Sanchez et al., 2011).
PA also plays an important role in adolescents’ mental health. Regular engagement in PA is associated with higher self-esteem, greater self-efficacy, and fewer internalizing symptoms, particularly during early adolescence (Laird et al., 2018; Wheatley et al., 2020). Importantly, PA often occurs in social context and can contribute to the development of social support, which is recognized as a protective factor for mental health in children and adolescents (Bauer et al., 2021). Despite these benefits, approximately 80% of adolescents worldwide do not meet PA recommendations, and recent evidence indicates a continuing global decline in adolescent PA levels (van Sluijs et al., 2021). At the same time, screen time is increasing, while many adolescents experience limited social support trends that collectively elevate the risk of physical and mental health problems (Inchley et al., 2020; Namysłowska, 2013).
Given these trends, promoting PA remains a major public health priority. However, the available evidence suggests that PA recommendations and intervention strategies may need to be tailored to individual social and behavioral contexts. This scoping review had an exploratory character; its purpose was to map practical recommendations and specific guidance that could inform the development of tailored PA strategies and potential intervention scenarios for adolescents with particular health concerns. Therefore, the aim of this scoping review is to synthesize and integrate PA recommendations for adolescents with overweight, high screen time, and/or low social support to identify shared principles for tailored PA interventions.
A scoping review methodology was adopted to identify and map the selected existing recommendations and guidance without undertaking a quantitative synthesis. Consistent with the objectives of scoping reviews, predefined research questions were not established. The review focused on the systematic identification and synthesis of recommendations and guidelines related to PA derived from completed interventions involving adolescents, with the purpose of informing the subsequent design of PA scenarios for selected risk groups. In addition, the review mapped the primary sources and types of evidence available in the literature concerning the effectiveness of solutions implemented in PA interventions targeting adolescents.
The methodological procedures followed the PRISMA Extension for Scoping Reviews (Tricco et al., 2018) (Figure 1). The review protocol was developed by the research team in accordance with the established reporting standards within the framework of the scientific project (project no. NdS-II/SP/0560/2023/01). The full protocol and supplementary materials are available from the corresponding author upon reasonable request.
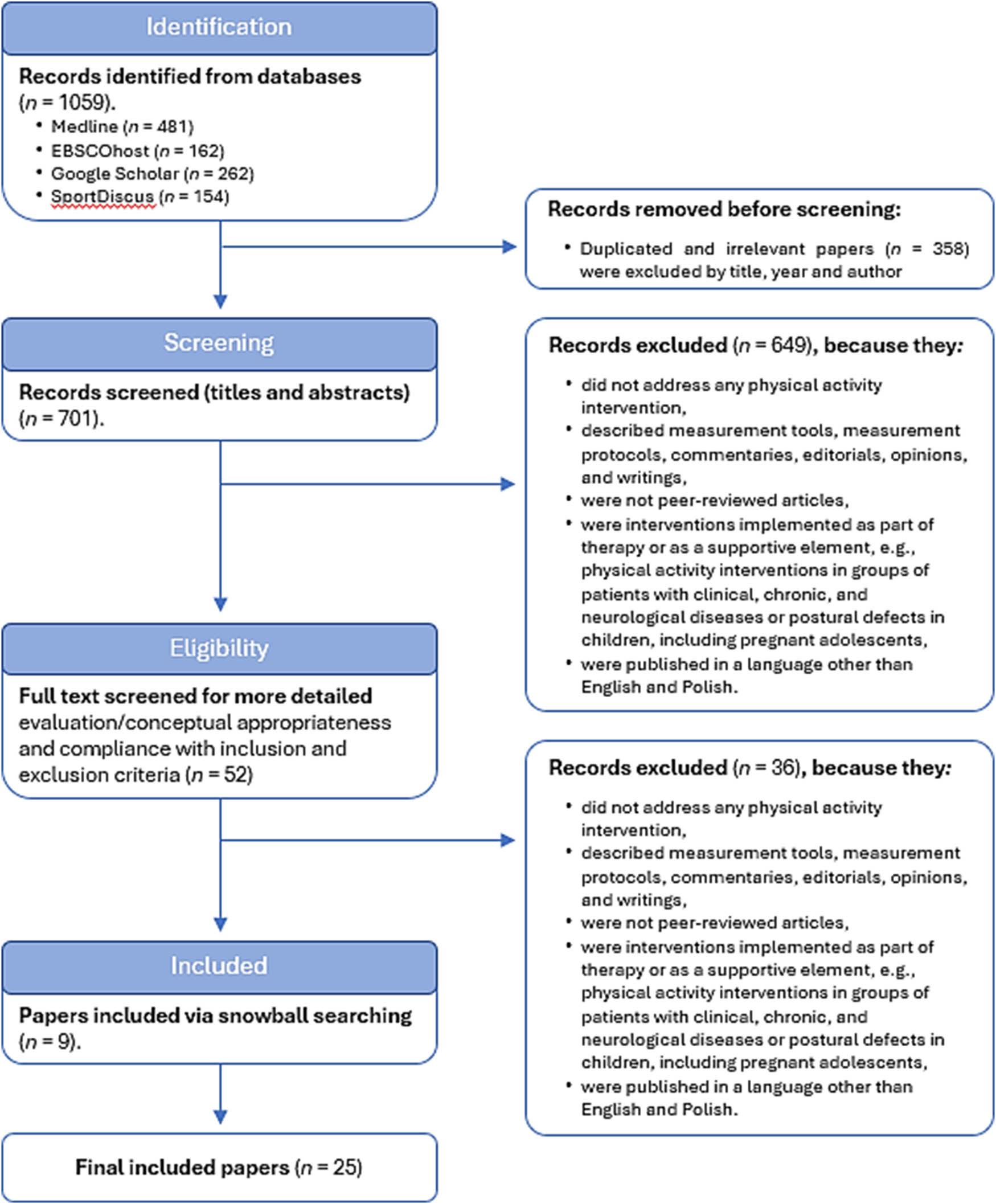
Flowchart of selection of studies
Relevant literature was searched in Medline (via PubMed), SPORTDiscus, EBSCOhost, and Google Scholar. A comprehensive strategy was applied to identify PA interventions targeting adolescents experiencing one or more of the co-occurring challenges described above. Search terms combined synonyms of “recommendations” AND (“physical activity of young people” OR “physical activity adolescents”) AND (“study” OR “intervention” OR “scientific research”) AND (“overweight” OR “obesity” OR “high screen time” OR “low social support”), adapted for each database. Reference lists of included articles were also screened for additional records.
The study was conducted using bibliographic databases, focusing on publications from January 2010 to August 2024. The search was limited to articles published in English or Polish, concerning adolescents aged 13–18 years.
Articles were considered eligible if they reported on PA interventions or recommendations recognized by researchers as most effective in addressing excess weight, reducing screen time, or enhancing social support among adolescents. Eligible studies could focus on various impact strategies. Additionally, studies reporting on implementation conditions of PA interventions considered most beneficial for addressing specific adolescent health issues were included. Studies were excluded if they did not provide an original contribution to the research topic or if the full text was unavailable (e.g., conference abstracts or meeting summaries).
The electronic databases were searched independently by one researcher (M.Ł.) using the predefined search strategy. A second reviewer (J.K.) conducted a blinded verification by screening 5% of titles and abstracts and 10% of full-text articles, achieving complete agreement (100%) with the initial screening results.
Data were extracted using a standardized template developed for this study. A deductive narrative synthesis was employed to summarize the themes and findings across the included studies. Consistent with the objectives of scoping reviews, no critical appraisal of methodological quality or risk of bias was conducted (Arksey & O’Malley, 2005; Tricco et al., 2018). However, missing information in articles was recorded in the data extraction template to assess overall methodological reporting quality. A meta-analysis was not undertaken due to the qualitative nature of most studies and the absence of predefined hypotheses.
The database search yielded 701 records after the removal of duplicates. Screening of titles and abstracts resulted in 52 articles being selected for full-text assessment. Of these, 25 studies met the inclusion criteria and were included in the qualitative synthesis. The final sample comprised 25 studies, including 5 meta-analyses. Key recommendations for the implementation of PA interventions among adolescents from specific risk groups are presented in Figure 2.
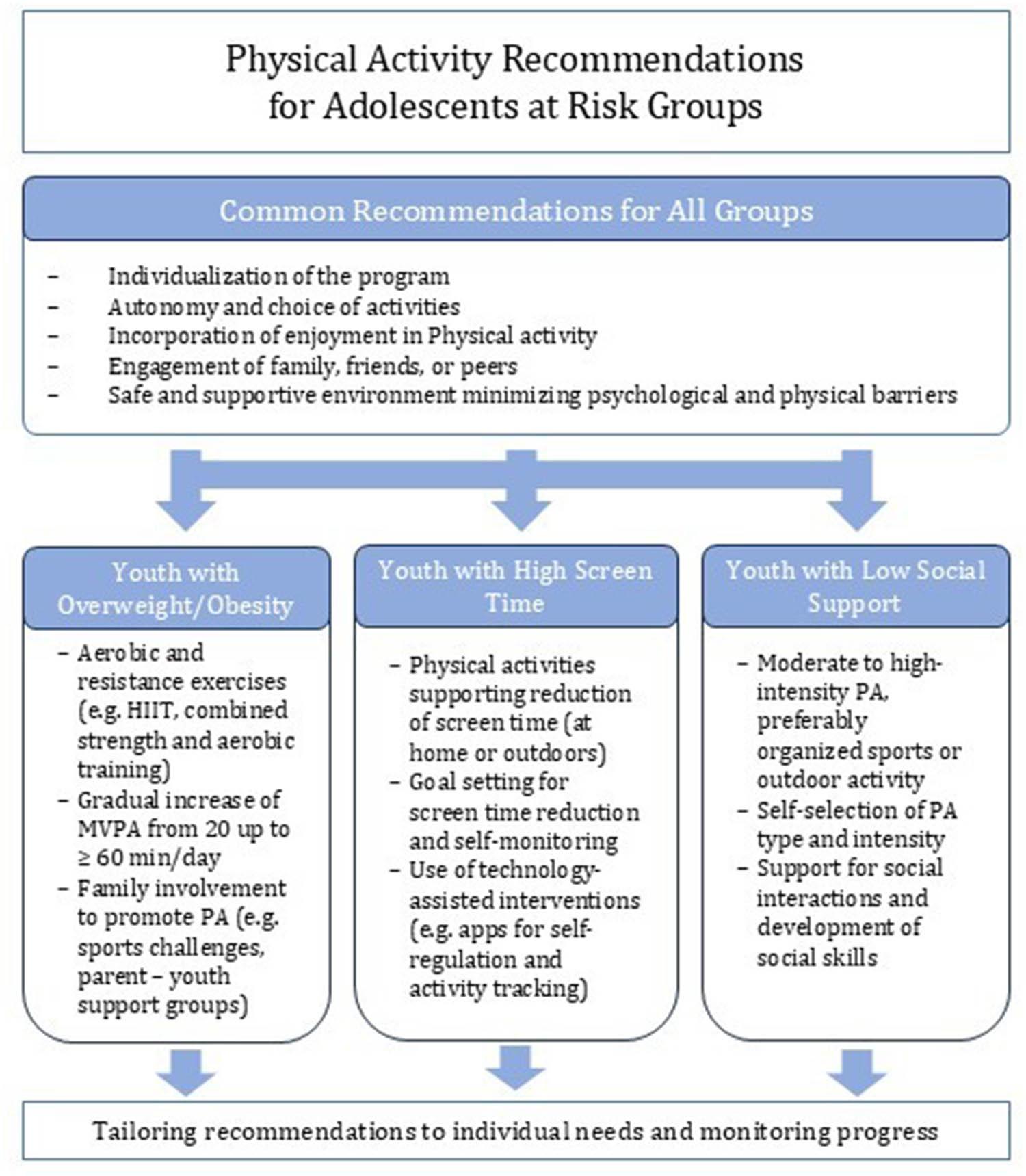
PA recommendations for adolescents in risk groups
Four main themes were identified: (1) the foundational role of the social environment; (2) barriers to PA among adolescents with health-related challenges; (3) matching training modalities to specific adolescent needs; (4) tailoring PA programs: main recommendations; and a multi-level, conceptual model (5) is proposed for integrated PA promotion in adolescents with overweight, low social support, and high screen time.
The existing literature consistently highlights the social environment as a central determinant of PA engagement and weight-related outcomes among adolescents (Chen et al., 2023; Hu et al., 2021; Tully et al., 2022; Yuan et al., 2025). Qualitative analyses indicate that family support, peer involvement, and community-level engagement play a pivotal role in facilitating behavioral change and sustaining PA participation (Chen et al., 2023; Tully et al., 2022). Interventions that actively involve families appear to be particularly effective for overweight and obese children and adolescents, as parents and caregivers are instrumental in implementing, reinforcing, and maintaining lifestyle changes over time (Tully et al., 2022). A child’s success in adopting more active behaviors is therefore closely linked to the capacity and commitment of the household to support these changes.
Peer relationships also represent a critical influence on PA behavior during adolescence. Evidence suggests that overweight and obese adolescents often form friendships with peers facing similar challenges, which may inadvertently reinforce sedentary behaviors (Chen et al., 2023; Salvy et al., 2012). However, these same social bonds can be leveraged within interventions to promote collective engagement in PA and enhance motivation through shared experiences (Chen et al., 2023). Community-based strategies, such as family sports days, group challenges, and parent–adolescent support groups, further strengthen these social mechanisms by fostering collective accountability and social connectedness (Chen et al., 2023).
Beyond social structures, individualization emerges as a key principle in effective PA promotion. Tailoring recommendations to adolescents’ social context, preferences, abilities, motivation, body awareness, and access to facilities enhances engagement and feasibility (Alberga et al., 2013; Chen et al., 2023; Tully et al., 2022). Physical and psychosocial characteristics interact to shape PA behavior, as illustrated by evidence indicating gender-specific motivational drivers in overweight adolescents – performance and strength among boys, and general health among girls (Alberga et al., 2013; Pescud et al., 2010). These findings underscore the importance of adopting a flexible, person-centered approach rather than uniform PA prescriptions.
A substantial body of evidence highlights psychosocial barriers as major impediments to PA participation in adolescents, particularly among those with health-related challenges (Khan et al., 2018; Moore et al., 2023; Wu et al., 2015). Anxiety, depressive symptoms, broader psychopathology, and poor sleep quality have all been identified as factors negatively associated with PA engagement (Khan et al., 2018; Wu et al., 2015). High screen time, in particular, appears to aggravate these challenges. Adolescents reporting more than 2 h of daily screen time and insufficient PA are more likely to experience psychosocial difficulties than their more active peers (Khan et al., 2018), a finding corroborated by evidence of both independent and interactive effects of low PA and high screen exposure on mental health outcomes (Wu et al., 2015).
Parental involvement plays a decisive role in mitigating excessive screen use (Ofcom, 2020; Zhang et al., 2022). Home-based interventions and those involving parents demonstrate greater effectiveness in reducing screen time among overweight and obese adolescents compared to peer-only approaches (Zhang et al., 2022). Similarly, adolescents with low levels of social support are less likely to meet PA guidelines, whereas strong encouragement from both family and peers is positively associated with daily and weekly PA engagement and participation in organized sports (Gill et al., 2018).
Autonomy also emerges as a critical psychosocial factor. Allowing adolescents to self-select the type and intensity of PA supports mental health by fostering autonomy, competence, and self-efficacy (Pascoe et al., 2020). Engagement in PA – particularly in socially supportive or nature-based environments – has been shown to improve body image, perceived competence, and social connectedness, all of which contribute to psychological well-being (Kondo et al., 2020; Pascoe et al., 2020). However, these potential benefits are increasingly undermined by persistently high levels of screen use. Contemporary data indicate that adolescents spend multiple hours per day engaging in online activities, television viewing, and gaming, with a marked increase over the past decade (Ofcom, 2020; Sikorska et al., 2021). This trend reinforces the need to address screen time as a distinct and interacting behavioral risk factor.
Evidence suggests that the effectiveness of PA interventions is enhanced when training modalities are aligned with the specific needs of different adolescent subgroups. For adolescents with weight management challenges, combined aerobic and resistance training appear superior to aerobic exercise alone in improving body composition, cardiometabolic markers, and fitness outcomes (García-Hermoso et al., 2018). Sequencing resistance training prior to aerobic exercise may further optimize outcomes, including improvements in VO2max and long-term PA adherence (Fiorilli et al., 2017). High-intensity interval training (HIIT) also shows promise as a time-efficient strategy, yielding significant improvements in blood pressure and aerobic capacity among overweight and obese adolescents (García-Hermoso et al., 2016).
For adolescents with high screen time, technology-based interventions may serve as an effective engagement tool rather than a competing risk. Smartphone applications designed to promote PA and reduce screen use have demonstrated high acceptability and perceived usefulness among adolescents (Direito et al., 2015; Lubans et al., 2014). However, the literature indicates that such tools are most effective when embedded within multi-component interventions that provide complementary social and behavioral support (Schoeppe et al., 2016).
Among adolescents experiencing low social support or mental health challenges, autonomy-supportive PA programs are particularly beneficial. Allowing participants to choose activity type and intensity enhances tolerance and engagement, even at higher intensities (Pascoe et al., 2020). Structured sport-based programs may also offer psychosocial benefits, supporting social integration and emotional well-being among at-risk adolescents (Lubans et al., 2012).
Despite the growing recognition of PA as a therapeutic and preventive strategy, the literature reveals a notable scarcity of comprehensive, group-specific recommendations for adolescents facing multiple, interacting health challenges (Aubert et al., 2021; Chaput et al., 2020). Nonetheless, several consistent principles emerge. Autonomy-supportive program design – offering meaningful choices and encouraging self-initiation – has been shown to enhance motivation and long-term adherence, particularly among overweight adolescents (Alberga et al., 2013; Deforche et al., 2011; Tully et al., 2022). Enjoyment and pleasure are equally critical, as positive affective responses to PA strongly influence sustained engagement (Angeles et al., 2024).
Current guidelines generally recommend at least an average of 60 min of MVPA per day, although evidence supports gradual progression from lower volumes, with even 20 min of regular aerobic activity producing meaningful reductions in body fat (Davis et al., 2011; Styne et al., 2017). Importantly, psychological comfort and environmental safety must be prioritized to reduce barriers related to weight stigma, embarrassment, and fear of injury (Alberga et al., 2013; Puhl & Luedicke, 2012). Access to supportive outdoor environments further facilitates PA engagement, whereas obesogenic neighborhood features, such as high fast-food density, may undermine intervention effectiveness (Hamano et al., 2017; Oreskovic et al., 2015).
Screen time reduction requires equally targeted strategies. Evidence indicates that interventions focusing specifically on screen use – rather than combining this aim with multiple health behaviors – are more effective in achieving sustained reductions (Andrade et al., 2015; Zhang et al., 2022). Goal-setting and self-monitoring appear particularly influential in modifying screen-related behaviors (Jones et al., 2021).
Based on the reviewed evidence and using the Bronfenbrenner’s socio-economic model (Bronfenbrenner, 2005), a multi-level, integrated conceptual model is proposed to guide future PA promotion interventions for adolescents experiencing overlapping challenges related to overweight, low social support, and excessive screen time.
At the individual level, the model emphasizes autonomy, enjoyment, and competence as core mechanisms driving sustained PA engagement. Interventions should allow adolescents to self-select activity type and intensity, align PA with personal goals (e.g., strength, health, social interaction), and incorporate progressive, achievable targets to enhance self-efficacy.
At the social level, family and peer support function as critical enablers. Parents and caregivers are positioned as co-regulators of behavior, supporting both PA participation and screen time reduction through modelling, encouragement, and environmental structuring. Peer-based strategies, including group activities and sport programs, foster social connectedness and reduce stigma, particularly for adolescents with low perceived support.
At the behavioral interface, PA promotion and screen time reduction are treated as interacting but distinct targets. Technology is reframed as a supportive tool rather than solely a risk factor, with digital applications facilitating self-monitoring, goal-setting, and feedback while limiting passive screen consumption. Structured PA modalities (e.g., combined aerobic–resistance training, HIIT, sport-based activities) are matched to individual needs and preferences.
At the environmental level, supportive physical and social contexts – including access to safe outdoor spaces, non-stigmatizing settings, and community-based opportunities – reduce psychological and practical barriers to participation.
Collectively, this integrated model conceptualizes PA behavior as the product of dynamic interactions between individual motivation, social support, behavioral regulation, and environmental affordances. Future interventions grounded in this framework may be better positioned to address the complex, co-occurring challenges of overweight, low social support, and high screen time among adolescents, thereby promoting sustainable improvements in both physical and mental health outcomes.
This review has several limitations that should be considered when interpreting the findings. Given the exploratory nature of a scoping review, the results should be interpreted as a mapping of existing guidance rather than as definitive, evidence-based recommendations. The absence of predefined research questions may have influenced the scope and structure of the search and data extraction processes. While the lack of predefined research questions allowed for a broad exploration of the literature, it may have affected the consistency and focus of the search and data extraction procedures. In addition, gray literature was not included, which may have resulted in the omission of relevant evidence. This may have resulted in publication bias and the under-representation of emerging or practice-based evidence. The review was restricted to studies published in English or Polish, potentially limiting the generalizability of the findings. Moreover, the included studies may be subject to potential risk of bias, primarily due to heterogeneity in study designs and the reliance on self-reported measures of PA and screen time. Despite these limitations, the synthesis provides a comprehensive overview of current recommendations and may serve as a foundation for future intervention studies aimed at promoting PA among at-risk adolescents.
This comprehensive review of the literature demonstrates robust evidence supporting the positive role of PA in addressing key health challenges among adolescents with overweight, high screen time, and low social support. While a substantial body of scientific and practical guidance exists for adolescents with above-normal body mass index, far fewer tailored recommendations are available for those experiencing excessive screen use or limited social support, highlighting an important gap in the literature.
For adolescents with overweight, the evidence consistently emphasizes the central role of family and peer support in facilitating and sustaining behavioral change (Chen et al., 2023; Tully et al., 2022). Effective PA interventions for this group require an individualized approach that accounts for social context, body awareness, personal interests, physical abilities, motivational factors, and access to appropriate infrastructure (Alberga et al., 2013; Chen et al., 2023; Tully et al., 2022). Autonomy-supportive strategies – particularly offering adolescents choice and encouraging self-selection of activities – are strongly associated with improved engagement and long-term adherence (Alberga et al., 2013; Deforche et al., 2011). Moreover, fostering enjoyment and pleasure during PA emerges as a key determinant of sustained participation (Angeles et al., 2024).
Reducing barriers to PA participation is equally critical. Psychological comfort, including protection from weight-related stigma, fear of injury, and unsafe or unsupportive environments, significantly influences adolescents’ willingness to engage in PA (Alberga et al., 2013; Hamano et al., 2017; Puhl & Luedicke, 2012). Evidence supports flexibility in implementation, including gradual progression and shorter activity bouts, particularly for adolescents with low baseline fitness (Styne et al., 2017). The literature further supports a range of training modalities for overweight adolescents, including combined aerobic and resistance exercise, resistance training followed by aerobic activity, and HIIT (Fiorilli et al., 2017; García-Hermoso et al., 2016, 2018).
In contrast, the evidence base for PA recommendations targeting adolescents with high screen time remains limited. Available studies suggest that addressing psychosocial barriers such as anxiety and depression is essential for promoting PA engagement (Khan et al., 2018; Wu et al., 2015). Parental involvement and home-based strategies are consistently identified as effective approaches for reducing screen time (Zhang et al., 2022). The use of digital tools designed to support screen time reduction and promote healthy behaviors appears promising, particularly when combined with goal-setting and self-monitoring strategies (Direito et al., 2015; Jones et al., 2021; Lubans et al., 2014). Importantly, interventions that focus explicitly on reducing screen time, rather than embedding this aim within broader lifestyle programs, demonstrate greater effectiveness (Andrade et al., 2015; Zhang et al., 2022).
For adolescents experiencing low social support, family and peer encouragement remains a critical determinant of PA participation (Gill et al., 2018). Engagement in natural environments and outdoor settings may further enhance motivation and social connectedness (Kondo et al., 2020). Autonomy in selecting activity type and intensity, alongside participation in at least moderate-intensity PA, appears particularly beneficial for this group (Pascoe et al., 2020). Structured sport-based programs focusing on a single discipline may also offer psychosocial and behavioral benefits (Lubans et al., 2012).
Overall, this review highlights that while evidence-based PA recommendations are well established for overweight adolescents, there remains a notable lack of integrated guidance addressing the combined challenges of overweight, excessive screen time, and low social support. Across all groups, the consistent determinants of successful intervention include family and peer involvement, individualized and autonomy-supportive program design, and attention to psychological comfort. The primary challenge for future interventions lies in sustaining long-term motivation and adherence, underscoring the need for integrated, multi-level PA promotion strategies that address both behavioral and contextual determinants of adolescent health.
The publication was co-financed from the state budget under the program entitled “Science for Society II” project no. NdS-II/SP/0560/2023/01, with a co-financing amount of PLN 475,172.50 and a total project value of PLN 475,172.50 (Poland).
Marlena Łopatka, Jana Krzysztoszek: Research concept and design, Collection and/or assembly of data; Marlena Łopatka, Michał Bronikowski, Małgorzata Bronikowska, Agata Korcz, Jana Krzysztoszek: Data analysis and interpretation; Marlena Łopatka, Michał Bronikowski, Małgorzata Bronikowska, Agata Korcz, Maryna Khorkova, Dagny Adamczak, Jana Krzysztoszek: Writing the article, Final approval of the article; Jana Krzysztoszek: Critical revision of the article.
The authors declare that they have no competing interests.