Neurosurgical patients may have external ventricular drains (EVD) inserted to monitor intracranial pressure (ICP). Additionally, these drains can be used to reduce elevated ICP in both emergent and urgent care scenarios, to protect against neurological infarction or herniation. EVD’s are also used following subarachnoid haemorrhage to aid in the removal of blood stained CSF, that can obstruct CSF reabsorption..
There are many causes of ventriculostomy associated infections (VAIs) and maintaining asepsis is the key to preventing negative patient outcomes. Neuroscience nursing collaboration worldwide is key to improving and maintaining standards of care. In 2024 at the Australasian Neuroscience Nurses Association (ANNA) conference, a workshop was facilitated to discuss practices and the care of patients with EVDs. This article explores the literature for evidence based practice and the differences in nursing management across Australasia.
Internationally neurosurgical nursing practices related to EVD’s varies based upon research findings, local guidelines, surgeon preference, historic practices and local experiences. Consequently, evidence based guidelines and education techniques also vary. These variations in practice may contribute to a range of risk factors for infection. Reviewing and adjusting guidelines may make a significant difference to reducing the risk of VAIs. Routine research and education is fundamental (Abraham, 2024). Research has found by utilising protocols or guidelines in education, standards of practice can be maintained over a period of 5 years (Hong et al, 2021).
The first External Ventricular Drain was developed in 1744 by Claude-Nicholas Le Cat and over time the technique and technology has evolved and in the later few decades infection rates have been the focus (Srinivasan et al, 2014). Indications for an EVD include (but are not limited to) brain tumour, traumatic brain injury (TBI), haemorrhage, hydrocephalus, or infection, and they can also be inserted in an emergency. The most commonly reported infections associated with EVDs are predominantly coagulase-negative staphylococci including Staphylococcus epidermidis and Staphylococcus aureus (Walek et al, 2022; Ståhlberg et al., 2025). However, with an increase in multi-drug resistant organisms, Acinetobactor baumannii, Klebsiella pneumoniae and Enterobactor spp are the most commonly reported Gram- negative bacteria (Bayston, 2019). While considered a common complication, the incidence of infection related to EVD and maintenance varies from 1.9% to 36% (de Andrade, Canicoba, Oliveira, Gnatta, & de Brito Poveda, 2024) - or 10–45% (Hepburn – Smith et al, 2015).
Risk factors contributing to VAIs are multifactorial (Walek et al, 2021; Sabnis et al 2020; Reiter et al 2023; Champey et al, 2018), however most are considered modifiable (de Andrade, et al, 2024). Nurses play a crucial role in risk mitigation by ensuring quality patient care in EVD management. Their responsibilities include: monitoring for signs of deterioration and or possible infection; maintaining targeted drainage goals whilst avoiding over-drainage or underdrainage; providing patient and family support and education; preventing infections; and ensuring prevention of accidental removal of the external ventricular drain. Ongoing education and promotion of guidelines is fundamental to ensure consistent best nursing practices and ensure high standards of care.
It is important to highlight the role of all health professionals, including those responsible for catheter insertion, in preventing infection. However, the nurse's unique role during handling and maintenance is especially critical for effective infection prevention de Andrade et al, (2024). Abraham (2024)) indicated 7 roles of the nurse in EVD management which included:
infection controller
wound care provider
team player
learner
educator
patient advocate
researcher
The authors highlight that ineffective practice can lead to infection, extended length of stay and complications such as worsening morbidity or death, this ensures staff remain vigilant. Health professionals must take all necessary steps to avoid a secondary health sequelae when managing EVDs.
This audit was considered a low risk notification and audit approval was sought. Eligible participants were informed of the nature of the audit by email and verbal communication at the conference, and given the opportunity not to participate. Consent was implied by completion and return of the questionnaire which was mentioned would contribute to a publication.
VAI’s pose a significant patient safety risk for patients with an EVD. There are also a variety of factors that can potentially impact the risk of VAIs; however it is difficult to identify the most fundamental factors associated with increased risk This includes and is not limited to: pre insertion hair removal (shaving of area for insertion); surgical preparation; catheter choice; surgical technique; dressing utilised; duration of dressing; care of insertion site; sampling technique and frequency of access to the sampling port; duration of EVD in situ; antibiotic use; patient and staff education; guidelines and staff techniques. Factors considered more likely to contribute to risk of infection include increased sampling frequency, exchange of EVD set, longer duration of catheter placement, and leakage from wound site (Hong et al, 2021; Khalaveh et al, 2023; Mehreen et al, 2022). Other factors not considered could include the immunity of the patient, co-morbidities and patient contact with the wound (Hepburn-Smith et al 2016).
Tunnelling of the EVD and prophylactic antibiotics were identified as significantly important to reduce the risk of infection (Hoefnagel et al., 2023). The efficacy of antimicrobial-impregnated and silver -impregnated ventricular catheters to reduce VAIs compared to plain catheters has been supported in the literature (Rienecker et al, 2023). However, the available antimicrobial-impregnated catheters contain active agents against gram positive pathogens, including the commonly occurring coagulase-negative Staphylococcus not the gram negative ones which might cause more severe infection (Karvouniaris et al., 2022).
Aneurysmal Subarachnoid Haemorrhage or fever with neuroinflammation within 2 weeks of EVD placement is indicative of a higher likelihood of non-infectious ventriculitis. Patients with arteriovenous malformation, alcoholism, or fever with neuroinflammation occurring after more than 3 weeks of EVD placement are more likely to necessitate antibiotic treatment for EVD infection. (Huang et al 2024). Another study by Zhu et al (2021) identified longer ICU stay, frequent CSF sampling, prolonged duration of EVD placement, and pre-operational intubation as independent risk factors for EVD infection. Bilateral placement of EVDs have no substantial influence on VAI risk.
A study by Walek et al (2021) over a 12 year period determined that the most important risk factors for reducing the risk of VAI were tunnelling of the EVD, reducing sampling frequency and alcoholic chlorhexidine cutaneous antisepsis. They also identified insufficient hair removal, dwell time, frequency of manipulation of the EVD, number of EVD insertions, and tract haemorrhage at placement as contributing factors for infection. Hypothesised factors that were not evidence based included: reduced GCS; age; raised intracranial pressure; length of hospital stay; involuntary disconnection; covering site with a dressing; blood in the drainage system; systemic infection and placement by a junior surgeon. By creating a care bundle with a committee and regular education and review they reduced EVD infections per 1000 EVD days from 6.68 (2007–2009) to 1.98 (2017–2019) which was a risk reduction of about 70% (Walek et al; 2021). Care bundles are important to ensure a standardised level of quality care aimed to prevent infection (Mehreen et al 2022; Lozano et al 2024; Ponnambath et al, , 2024).
Developing a culture of safety within the interdisciplinary team providing education and a guideline, minimising handling, changing dressings only when compromised and stopping routine access of the system to collect samples for cultures, are important factors to reduce the risk of VAI (Sabnis et al (2020); Reiter et al (2023) and Champey et al (2018)). Studies also have identified insertion site cleaning with chlorhexidine, dressing change only when indicated and use of Biopatch TM at insertion site is associated with less VAIs (Langhorne and Heitschmidt, 2024).
Internationally Aseptic Non Touch Technique (ANTT) is the global standard for safe and efficient asepsis management (Chen at al., 2024). There are two types, surgical and standard. The standard or surgical technique includes 6 steps which are risk assessment, environmental management, decontamination and protection, aseptic field selection and management, non touch technique and infection prevention. The standard ANTT method includes protection of key parts and protection of individual key sites, a mandatory non-touch technique and either the use of no gloves or non-sterile gloves. Surgical ANTT includes key part protection on a collective sterile field, sterile gloves are essential and non-touch technique is desirable. Whilst EVD sampling is not included in these guidelines, a surgical technique is essential to prevent infection and avoid touching key parts. The utilisation of sterile gloves ensures key parts are not compromised.
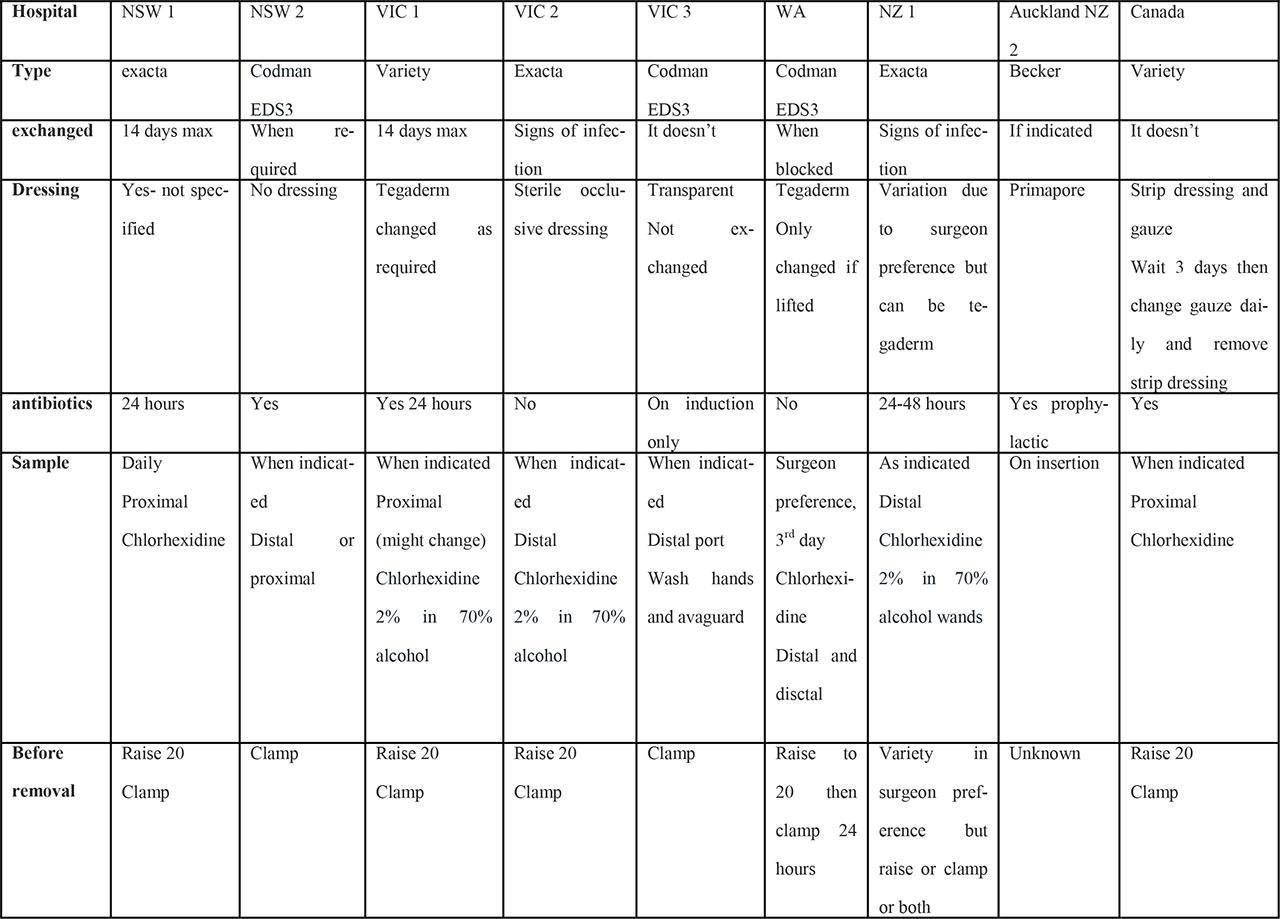
The workshop included neuroscience nurses from across Australasia, with special guests from Canada. From within Australasia, we had representatives from Western Australia (WA), New South Wales (NSW), Victoria (VIC), Auckland (NZ), Wellington (NZ) and Queensland (QLD). A range of nurses had completed a pre-workshop questionnaire of which the findings can be viewed in table one (n = 9). The EVD systems in use included Medtronic Exacta (n= 3), Codman EDS3 (n = 3), Medtronic Becker (n= 1). Two centres had a variety of products due to a lack of availability. Participants in the workshop discussed risk factors including the handling of the EVD on ward rounds, unnecessary touching of the EVD or scratching of the wound by the patient or cleaning of hands with alcohol gel prior to emptying the burette every hour, which is often not discussed in the literature.
One hospital in NSW used no dressing but the rest used a dressing (n=8). EVDs sites were dressed with clear dressings (n = 5) or dry dressings (n = 2) or gauze and strip dressing (n = 1), one was not specified, and one used a variation in dressings due to surgeon preference. An EVD site dressing provides a physical barrier which is beneficial to prevent touching of the wound. The benefits to a clear dressing are that the wound can be sited through the dressing so the dressing does not have to be removed but the limitation is precipitation, although chlorhexidine discs can assist with this problem and only one study has reviewed this with a low number of participants (Hepburn-Smith et al 2016; Roethlisberger et al, 2018).
Occlusive dressings are easier to remove and replace if soiled but are likely to come off due to lack of hair removal or because they are less able to stick to the wound. A small study identified that occlusive dressings were not necessary and a 10cm patch of hair was shaved prior to surgery for preparation (Catapano et al, 2019). No centres in the project utilise a skin glue such as 2 octyl cyanoacrylate dressings which one small study (n= 259) showed that these glues were superior to standard occlusive dressings (Brookland et al, 2014). Another small study (n = 179 EVDs) assessed their own EVD guideline over a 7-year period and reported one infection in a patient with delirium who removed their own EVD. They did not explain their sampling technique but reported they did shaved a large area and utilized an occlusive clear dressing with a chlorhexidine disc and also tape around the edge of the dressing with weekly dressing changes (Flint et al, 2017).
Frequent changes in EVDs used to be common practice but this has changed due to studies that have demonstrated the reduction in VAI maintaining the same catheter (Katzir et al (2019); Wong et al (2002). However, a study by Huang et al (2024) reported the risk of VAI is higher in patients with an EVD dwell time >14 days Hence, some practice variations were reported in Australasia with most centres now only exchanging them if indicated due to signs of infection (n=5) or at 14 days (n=2) or not exchanged at all (n=2). 7 out of the 9 centres were using prophylactic antibiotics for 24–48 hours or on induction.
Research indicates that sampling should only take place when clinically indicated and sampling frequency should be reduced to prevent VAIs (Walek et al, 2021; Sweid et al (2020) and Catapano et al (2019). Hoefnagel et. al (2023) recommend sampling at the time of insertion, when infection is suspected, 48–72 hours after initiation of antibiotic treatment and upon removal of the EVD.
Sampling techniques varied and included sampling from the distal (n = 5), or proximal port (n= 3), or both the proximal and distal ports (n = 1). Kinast et al (2022) determined that the proximal port can increase the risk of infection. The distal port has been described as being as good as the proximal port (Hepburn-Smith et al (2016); Wong (2011). Additionally, whilst the collection bag has been described as a possible sample site, unless the bag is changed daily this would provide is an old sample of CSF and changing the bag more frequently might then contribute to another risk of infection (Khalaveh et al (2023) and Kinast et al (2022)). All centres were using chlorhexidine 2% and 70% alcohol but a variety of product types are being utilised. Most centres use wipes but one centre utilised wands. Most centres have a range of practices due to surgeon preference with raising and or clamping prior to removal of the EVD.
There are also a range of practices for sampling the EVD. Shani & Krishnakumar (2023) recommend dripping one millilitre out rather than using a syringe to remove the cerebral spinal fluid and put into a sterile container for collection. This was the practice of some of the nurses at the workshop, a technique whereby CSF was collected from the distal port through a filter (Kinast et al, 2022). In a trial of a care bundle in Korea, a significant reduction in EVD infections was achieved by sampling via a closed system. It recommended sampling should occur from the three way tap using a swab wand (Choo et al, 2023). In another study of patients with subarachnoid haemorrhage, the proximal port is doused in providone Iodine for 3 minutes using 3 swabs, a total of 1 swab per minute and allowed to dry, then sampling is completed using a needle and syringe (Catapano et al, 2019). Using a syringe to take out the CSF from the proximal port may be more risky than the distal port because if fluid is drawn too quickly or insuffient fluid this could remove brain tissue with the sample.
There are a variety of practices regarding swabbing and drying but there is limited research on optimal swabbing and drying times. Both are important and ANTT recommends scrubbing the hub, not just dousing the sample port with alcohol but actually scrubbing the site. Exact timing has not been established for EVD sampling although timing for other hubs are 15–20 seconds with a drying time of the same (Chen at al., 2024). One study looked at patients having stem cell transplants with low immunity and high risk for infection and concluded longer scrubbing time decreases line contamination and 60 seconds scrubbing was the best outcome and required at least 30 seconds drying time (Alonso et al 2019). Drying time is important to consider and ensure this is calculated and researched. Poor sampling technique can lead to the introduction of microbes into the system or contamination of the sample (Lenski et al, 2019; Talibi et al, 2020).
There are many contributing factors to increase the risk of VAIs and therefore it is important to consider all aspects of care to reduce the risk of VAI’s (table 2).
Factors to consider for reduction of the risk of VAIs
| Technique factors | Personal factors |
|---|---|
| Insertion technique | Patient scratching the wound |
| Tunnelling recommended | Confused pt touching the EVD /EVD site. |
| Type of catheter | Patient dislodging or removing the drain |
| Antibiotic impregnated or non-antibiotic impreg- | |
| Dressing used | Patient removing the dressing |
| Clear dressing with chlorhexidine disc and tape around outside with dressing changed every 7 days. | |
| Or assess the use of 2 octyl cyanoacrylate glue | |
| Sampling technique | Minimise touching of drain or wound |
| Port - distal | |
| Drip method | |
| Closed system syringe method | |
| Open system syringe method | |
| Sterile field | |
| Sterile gloves | |
| 2% chlorhexidine and 70% alcohol – wand or swab | |
| Gel hands or wear gloves when touching the wound or drain | To avoid cross contamination and reduce the risk of infection |
When making changes to practice it is important to examine the research, discuss the practice options with all relevant stakeholders, including nursing and medical colleagues both locally and internationally, significant trade representatives, infection control and line management colleagues. Guidelines do not have to change extensively but they should be reviewed and where necessary changes made to the management of EVDs if contemporary high standards of care is to remain current. . Care bundles are key, although it is difficult to determine the most important factors to prevent infection as there are many potential contributing risk factors.
In conclusion, the key recommendations for neurosurgical teams to consider include:
The insertion techniques and catheter selection
Dressings types and frequency of dressing changes
Prophylactic antibiotic use
Sampling techniques and frequency
Unnecessary touching of the EVD or wound site.
Unnecessary touching of the EVD or wound site is an important risk factor for infection. Recommendations include reducing the frequency of sampling and reviewing local, area-specific guidelines to support infection prevention. The collaborative discussions at the workshop—attended by neurosurgical nurses from at least nine different hospitals across Australasia—highlighted shared challenges and potential improvements. By refining our guidelines and strengthening education, we can work together to enhance standards of EVD care and potentially reduce infection rates. Ensuring the gelling of hands prior to touching the EVD each hour is an important consideration. Particular attension for nurses could be regarding the aseptic technique to dressings and sampling. Dressings or lack of dressing and cleaning of the wound are fundamental considerations Furthermore, the sampling technique including scrubbing and drying times are important focus areas for nurses. Further research into the optimal dressing and wound care is fundamental.
What adjustments will you do to improve your practice or the practice of those in your team to improve your practice?
Review of hospital in Australasia EVD techniques