
Multiple sclerosis (MS) is a chronic, neurodegenerative, inflammatory, and demyelinating disease of the central nervous system (CNS) that damages myelin sheaths, oligodendrocytes, nerve cells, and axons. It is characterized by a gradual and progressive limitation of functional ability, leading to disability, especially in younger people aged between 20 and 40 years [1]. The main cause of MS remains unidentified, but it is believed to be an autoimmune disease [2,3]. Worldwide, prevalence rates range from 15 to 180/100,000 people; in Poland, they ranged from 45 to 92/100,000. The incidence rates vary depending on geographical distribution: in Europe they range from 3.5 to 5.5/100,000, in Poland, they range from 2.4 to 4.3. MS affects women more often than men [4,5,6,7].
The widely accepted view of the immunopathogenesis of MS in humans suggests that myelin-specific autoreactive T cells are activated in the peripheral immune system through the interplay of environmental factors and genetic susceptibility. The exact mechanisms of autoreactive T cell activation remain unknown but may occur because of nonspecific polyclonal activation by bacterial or viral antigens [8,9]. Additionally, a structural homology between host and pathogenic proteins could cause autoimmune reactions [10]. Once activated, T cells acquire the potential to cross the blood-brain barrier. This process is driven by the expression of integrins on the cell surface of inflammatory cells, which mediate their binding to the vascular cell adhesion molecule (VCAM-1) expressed on capillary endothelial cells. VCAM-1 expression is induced by tumor necrosis factor necrosis factor alpha (TNF)-α and interferon gamma (IFN)-γ during inflammation. Matrix metalloproteinases (MMPs) are released by T cells to facilitate their passage through the extracellular matrix. MMPs are also involved in the subsequent degradation of myelin components [4,11]. Activated T cells break myelin, releasing new CNS antigens. The cascade of proinflammatory cytokines and the recruitment of additional inflammatory cells and specific B lymphocytes produce myelin antibodies at the site of inflammation, which additionally contribute to tissue damage [12,13]
Periodontitis is characterized by the progressive deterioration of the tissue supporting the teeth [14,15], as chronic inflammation associated with opportunistic bacterial microflora is a source of bacteria, that can potentially influence MS occurrence as well as other neurodegenerative diseases [16]. The presence of bacteria in periodontal tissues leads to the development of chronic inflammation, as well as the release of their metabolic products and mediators of the immune reaction into the bloodstream. As a result of an inflammatory reaction in the periodontium, inflammatory mediators, metalloproteinases, prostaglandins, eicosanoids, kinins, cytokines, chemokines, and complement activation products are released into the circulation [17,18].
To date, only a few studies assessing the oral cavity condition of patients with MS have been conducted, and only two studies have assessed the association between MS and periodontitis in humans [19,20]. Only one questionnaire study has been conducted in the Polish population. It showed dry mouth and gingival bleeding are most common symptoms in more advanced types of MS [21].
Mouth dryness might also be found as an element of other conditions [22,23,24]. However, xerostomia can develop as an adverse effect of certain medications. More than 500 drugs can cause or increase mouth dryness [23,25].
Due to the limited number of studies conducted to date, we focused on the expanded knowledge of the oral health status of MS patients.
The aim of this study is to comprehensively evaluate the oral health status of patients with MS, with particular emphasis on periodontal condition, oral hygiene indices, and the prevalence of xerostomia. Additionally, the study explored potential associations between oral health parameters and clinical characteristics, including disease duration and neurological disability as assessed by the expanded disability status scale (EDSS) score.
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Poznan University of Medical Sciences (Resolution No. 314/16 on March 3, 2016 and 1300/18 on Decembre 6, 2018). Written consent to participate in the study was obtained from all the subjects.
The sample size was calculated in accordance with the selection of a representative sample of the inhabitants of Poznan.
A total of 230 MS hospitalized patients at the Independent Public Healthcare Center (PHC) of the Ministry of Interior and Administration in Poznan were examined. Forms of MS other than relapsing-remitting MS (RRMS), toothlessness, and pregnancy were exclusion criteria from the study. Finally, the study group consisted of 170 patients: 123 women and 47 men aged 26–66 years, with an average age of 42.6 years (Table 1). All patients were treated with immunomodulating therapy according to the PHC hospital protocol with the following drugs: IFN beta-1a (N = 53), IFN beta-1b (N = 37), dimethyl fumarate (N = 47), glatiramer acetate (N = 19), teriflunomide (N = 6), fingolimod (N = 7), and cladribine (N = 1).
Baseline characteristics of the study group and control subgroup
| Variable | MS group (n = 170) | Control group (n = 50) | p-value | |
|---|---|---|---|---|
| Sex | Female | 123 (72.4%) | 99 (66.0%) | 0.39 |
| Male | 47 (27.6%) | 51 (34.0%) | ||
| Age | <30 years | 18 (10.6%) | 30 (20.0%) | |
| 30–50 years | 113 (65.5%) | 90 (60.0%) | ||
| >50 years | 39 (22.9%) | 30 (20.0%) | 0.29 | |
| Education | Primary | 4 (2.4%) | 6 (4.0%) | |
| Vocational | 17 (10.0%) | 27 (18.0%) | ||
| Secondary | 67 (39.4%) | 42 (28.0%) | ||
| Higher | 79 (46.5%) | 75 (50.0%) | 0.41 |
The control group included 150 random patients, 99 healthy women and 51 healthy men aged 21–72 years, from the General Dental Clinic: Poznan University of Medical Sciences. Patients attending a dental check-up were included in the control group.
The oral cavity of all participants was assessed via a dental mirror and a WHO 621 periodontal probe. All patients were examined by one researcher – a periodontist. Oral hygiene was assessed via the approximal plaque index (API), gingival bleeding was assessed via the modified sulcus bleeding index (mSBI), and general periodontal status was determined via the community periodontal index of treatment needs (CPITN). These simple indices were chosen for clinical examination of hygiene levels and the presence of active infection because MS patients were examined in the medical ward.
The API assesses the presence or absence of plaque in interdental spaces. The index value was calculated by dividing the sum of the interdental spaces containing the plaque by the sum of all assessed interdental spaces. The evaluation criteria were as follows: 70–100% – poor hygiene; 40–69% – average hygiene; 25–39% – rather good hygiene; <25% – optimal oral hygiene [26].
The mSBI assessment was based on the presence or absence of bleeding during the insertion of a periodontal probe into the gingival sulcus in the interdental spaces. The value of the index was calculated by dividing the sum of bleeding gingival units by the sum of all gingival units tested. MSBI values were interpreted as follows: 50–100% – severe gingivitis; 30–49% – moderate gingivitis; 10–29% mild gingivitis, and <10% clinically healthy gingiva [27].
Periodontal probing depth (PPD) measurements were also taken to assess whether the patient had periodontal disease. Because measurements were done at the hospital ward, for the purposes of this study, according to the recommendations of Page and Eke [28], periodontitis was diagnosed on the basis of the presence of PPD >4 mm on two nonadjacent teeth.
Each patient was diagnosed according to the CPITN criteria to determine the periodontal status of each dentition segment. The codes used for this indicator have the following values: code 0: periodontal health; code 1: gingival bleeding during probing; code 2: deposits and bleeding; code 3: periodontal pocket 3.5–5.5 mm; and code 4: periodontal pocket ≥ 5.5 mm [29].
On the basis of the data from the examination, patients were classified in terms of periodontal status into one of three groups: healthy periodontium, gingivitis, and periodontitis.
To assess mouth dryness, the mirror test was performed: the back of a dental mirror was moved across the inside of the buccal mucosa immediately after opening the mouth when the oral inspection was started. If the dental mirror was sticking to the mucosa, friction was noted.
The survey questionnaire included information on age, sex, place of residence, education, other chronic diseases, medications used, and smoking. Patient cards provided information on the duration of the disease, as well as the value of the EDSS, which is used to assess the progression of motor disability in MS patients. The EDSS was assessed by a neurologist within 3 months before the oral examination.
EDSS is a method of quantifying disability in MS patients and monitoring changes in disability levels over time. It is widely used in clinical trials and in the evaluation of people with MS. It was developed by neurologist John Kurtzke in 1983, and the EDSS ranges from 0 to 10 in increments of 0.5 units. Values from 1.0 to 4.5 refer to people who can walk without any help, while values from 5 to 9.5 refer to people with mobility problems [30].
The calculations were performed via Statistica 13 (TIBCO) and PQStat software. The level of significance was α = 0.05. The result was considered statistically significant when p < 0.05. Sample size calculations were performed with confidence level of 95% and a margin of error of 7.5%. The normality of the distribution of variables was tested with the Shapiro–Wilk test. To compare the variables between the two groups, in the case of compliance with the normal distribution and equal variance, Student’s t-test was used for unrelated samples; in the case of noncompliance with the normal distribution, the Mann–Whitney test was used. An analysis of variance test for samples unrelated to Tukey’s multiple comparison test or the Kruskal–Wallis test with the Dunn–Bonferroni multiple comparison test was computed to compare the variables between multiple groups. To test the relationships between the variables, the chi-square test of independence, the Fisher exact test, or the Fisher–Freeman–Halton test were used. The correlations were determined via the Spearman correlation coefficient.
The periodontal status of the patients in the study group was as follows: 61% had healthy periodontium, 30% had gingivitis, and only 9% had periodontitis (Table 2). In the control group, the corresponding values were 50, 24, and 26%, respectively. These differences reached statistical significance (p = 0.027), suggesting a higher prevalence of periodontitis in the control group.
Data comparison between the study group and the control group
| Study group | Control group | p-value | ||
|---|---|---|---|---|
| Periodontal status | Healthy | 104 (61%) | 75 (50%) | 0.027 |
| Gingivitis | 50 (30%) | 36 (24%) | ||
| Periodontitis | 16 (9%) | 39 (26%) | ||
| Periodontal status using CPITN | CPI = 0 | 49 (28.8%) | 42 (28%) | 0.059 |
| CPI = 1, 2 | 103 (60.6%) | 75 (50%) | ||
| CPI = 3 | 16 (9.4%) | 24 (16%) | ||
| CPI = 4 | 2 (1.2%) | 9 (6%) | ||
| mSBI | Mean value | 11.84% | 15.33% | 0.086 |
| API | Mean value | 32.59% | 45.85% | p < 0.001 |
| Hygiene according to API | Bad | 10 (6.06%) | 30 (20%) | p < 0.001 |
| Average | 33 (20%) | 57 (38%) | ||
| Rather good | 50 (30.3%) | 33 (22%) | ||
| Optimal | 72 (43.64%) | 24 (16%) | ||
| Teeth number | Mean value | 25 | 25 | 0.613 |
| Dry mouth incidence | 83 (49%) | 8 (16%) | p < 0.001 |
When periodontal status was assessed using the CPITN index, no statistically significant differences were observed between the groups (p = 0.059), although the result was close to the threshold of significance. In the study group, CPI = 0 was observed in 28.8% of patients compared to 28% in the control group. CPI codes 1 and 2 were more frequent in the study group (60.6% vs 50%), whereas higher CPI scores (3 and 4), indicating more advanced periodontal disease, were more common in the control group (22% vs 10.6%).
The differences between the classification methods may result from the diagnostic criteria used. In the present study, gingivitis was defined as bleeding on probing in more than 10% of interdental sites, whereas CPITN code 1 is assigned even in the presence of a single bleeding site.
Oral hygiene, assessed using the API index, was significantly better in the study group. The mean API value was 32.59% in the study group and 45.85% in the control group (p < 0.001). Optimal hygiene was more frequently observed in the study group (43.64% vs 16%), while poor hygiene was less common (6.06% vs 20%) (p < 0.001).
The mean mSBI value was lower in the study group (11.84%) compared to the control group (15.33%), although this difference did not reach statistical significance (p = 0.086).
There were no significant differences in the number of teeth between the groups, with a mean value of 25 teeth in both groups (p = 0.61).
Differences between groups for categorical variables were analyzed using the chi-square test, while continuous variables were compared using the Student’s t-test depending on data distribution.
A statistically significant difference was observed in the prevalence of xerostomia. Dry mouth was detected in 49% of patients in the study group compared to 16% in the control group (p < 0.001), indicating a markedly higher prevalence in the study group.
No significant association was found between periodontal status and gender (p = 0.318). However, periodontal status was significantly associated with age (p = 0.002), with gingivitis and periodontitis more frequently observed in older patients. A strong association was also found with education level (p < 0.001), as patients with higher education more often presented with a healthy periodontium. No significant relationships were found for place of residence (p = 0.306) or smoking status (p = 0.609).
The mean EDSS score was 1.7 (median: 1.5), and the mean disease duration was 9.3 years (median: 9 years). Correlation analyses were performed to assess the relationships between EDSS score, disease duration, and oral health parameters, including API, mSBI, and the number of teeth (Table 2).
No statistically significant correlations were found between disease duration and any of the analyzed oral health parameters. The correlation coefficients were low and non-significant for API (r = 0.092, p = 0.238), mSBI (r = 0.018, p = 0.823), and number of teeth (r = −0.142, p = 0.069), indicating no meaningful association.
In contrast, statistically significant correlations of moderate strength were observed between EDSS score and all analyzed oral health parameters. A positive correlation was found between EDSS and API (r = 0.352, p < 0.001), as well as mSBI (r = 0.330, p < 0.001), indicating that greater neurological disability was associated with poorer oral hygiene and increased gingival bleeding.
A negative correlation was observed between EDSS score and the number of teeth (r = −0.4, p < 0.001), suggesting that higher disability was associated with a lower number of preserved teeth.
Overall, these findings indicate that functional impairment, as measured by EDSS, is significantly associated with worse oral health outcomes, whereas disease duration alone does not appear to be a significant factor (Table 3).
Values of Spearman’s correlation coefficient depending on disease duration and the EDSS score according to the API, mSBI, and number of teeth
| Variable | Value of the Spearman’s correlation coefficient | |
|---|---|---|
| Disease duration | EDSS | |
| API | 0.092 (p = 0.238) | 0.352 (p < 0.001) |
| mSBI | 0.018 (p = 0.823) | 0.330 (p < 0.001) |
| Teeth number | −0.142 (p = 0.069) | −0.400 (p < 0.001) |
Dry mouth was reported by 83 patients (48.8%). No statistically significant associations were found between the occurrence of xerostomia and gender (p = 0.718).
A significant association was observed with age (p < 0.001). The prevalence of dry mouth increased markedly with age, affecting 71.79% of patients over 50 years, 46.49% of those aged 30–50 years, and only 11.76% of patients under 30 years of age.
A statistically significant relationship was also found between xerostomia and education level (p < 0.001). Dry mouth was most frequently observed among patients with vocational education (71.74%), compared to those with secondary (52.24%) and higher education (35.44%), indicating a decreasing trend with increasing education level.
Furthermore, the type of disease-modifying therapy was significantly associated with the occurrence of dry mouth (p = 0.01147). Xerostomia was most commonly reported among patients treated with IFN beta-1a (66%) and IFN beta-1b (57%), whereas lower prevalence was observed in patients receiving dimethyl fumarate (34%) and glatiramer acetate (32%) (Figure 1).
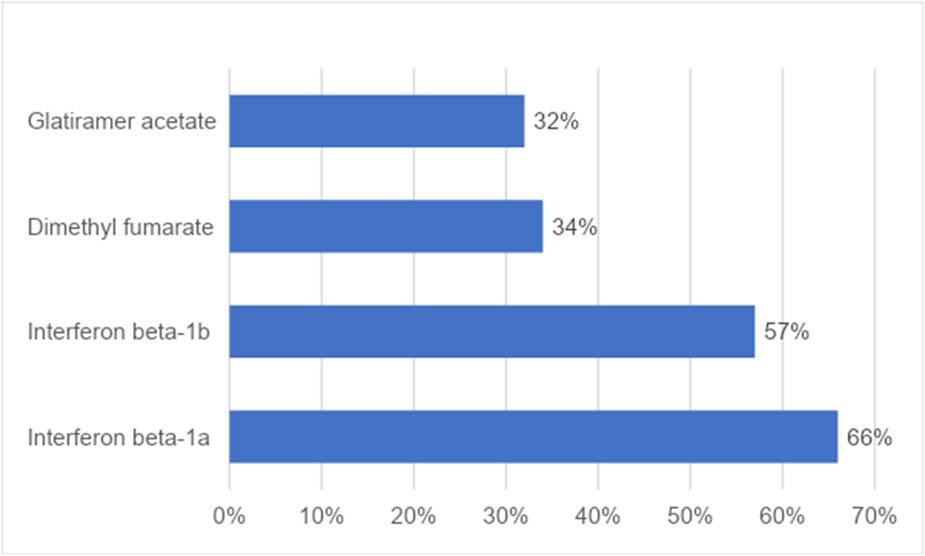
Percentage of patients reporting dry mouth according to the type of treatment
Overall, these findings indicate that xerostomia is strongly associated with age, education level, and type of treatment, but not with gender.
The condition of the periodontium is known to vary with age and may be influenced by multiple factors, including the presence of systemic diseases, reduced manual dexterity, and differences in health awareness [31,32].
In the present study, there was no association between MS and periodontitis. On the contrary, periodontitis was significantly less prevalent in the MS group compared to the control group. This aspect is particularly interesting when considering the treatments received by patients, as many medications used in MS therapy may adversely affect periodontal status [33]. This finding contrasts with some of the available publications and therefore requires careful interpretation [34,35].
One possible explanation for this result is the significantly better oral hygiene observed in the MS group, as reflected by lower API values and a higher proportion of patients with optimal hygiene. It may be hypothesized that patients with chronic diseases, such as MS, remain under continuous medical supervision, which could promote greater health awareness and adherence to preventive behaviors.
Only a limited number of studies have evaluated periodontal status in MS patients, and most available meta-analyses are based on a small number of clinical studies [34]. Our findings differ from some previous reports; however, methodological differences between studies should be considered.
A large case-control study demonstrated no association between MS and periodontitis after adjustment for smoking and other variables [20]. Similarly, an analysis conducted in a Spanish population revealed heterogeneous periodontal findings, although standardized periodontal indices were not applied [35].
Other studies based on the questionnaire data reported the high prevalence of gingival bleeding among MS patients; however, these findings were not significantly associated with disease activity or treatment [36]. Population-based data from Taiwan suggested an association between MS and periodontitis, although these results were based on administrative databases without clinical examination [19]. Also, poor oral health was declared by 22% of the 1,523 Australian MS respondents, which was higher than that reported by the general adult population in Australia [37].
Differences between studies may result from variations in the study design, diagnostic criteria, and population characteristics. It may also be considered that immunomodulatory therapies used in MS patients could influence inflammatory responses and potentially modify the course of periodontal disease.
The oral hygiene of the MS patients in this study was better than that of the control group. This finding may appear unexpected, as neurological impairment could theoretically limit the ability to maintain proper oral hygiene.
However, patients with chronic diseases are often more frequently in contact with healthcare professionals, which may increase their awareness of general and oral health. Additionally, preventive recommendations provided during medical care may contribute to better hygiene practices.
It should also be noted that most available studies assessing oral hygiene in MS patients rely on self-reported data rather than objective clinical indices, which makes direct comparison difficult.
One study on a group of 101 patients reported that 50% of participants assessed their hygiene as good, while 26% described it as sufficient [38]. However, these results were based on self-reported data, which may not accurately reflect actual oral hygiene status.
The number of teeth is an important indicator of long-term oral health. In the present study, no significant differences were observed between the study and control groups in this parameter. This finding contrasts with previous reports suggesting increased tooth loss in MS patients [39,40]. These discrepancies may be explained by differences in disease severity, access to dental care, and the characteristics of the studied populations.
In the present study, a significant relationship was observed between neurological disability, as measured by the EDSS score, and oral health parameters. Higher EDSS scores were associated with poorer oral hygiene, increased gingival inflammation, and a lower number of teeth. These findings are consistent with previous reports indicating that patients with greater physical disability present worse periodontal parameters and increased tooth loss [41].
The observed associations may be explained by reduced manual dexterity, impaired motor coordination, fatigue, and other neurological symptoms such as tremor or ataxia, which can significantly affect the ability to perform effective oral hygiene procedures [42,43]. However, it should be noted that not all studies confirm this relationship [35].
Dry mouth is a common problem in MS patients and may be caused not only by the disease itself, but also by drugs used to treat MS. Xerostomia is one of the most frequently reported adverse effects of medications used in MS and may be associated with additional symptoms such as dysgeusia, dysphagia, and mucosal lesions [44].
In the present study, xerostomia was reported by nearly half of the patients and was significantly more prevalent than in the control group. The occurrence of dry mouth was associated with age, education level, and type of treatment. In particular, a higher prevalence was observed among patients treated with IFN beta-1a and beta-1b, which may be related to mechanisms typical of autoimmune responses and treatment-related side effects [45].
These findings are consistent with previous reports indicating a high prevalence of xerostomia in MS populations [37]. Reduced salivary flow has also been demonstrated in MS patients in other populations, suggesting that both subjective and objective mechanisms may be involved [39].
The results of the present study suggest that xerostomia is an important clinical problem in MS patients and should be taken into account in their comprehensive care.
Several limitations of this study should be acknowledged. First, the diagnosis of periodontitis was based solely on clinical examination without radiological assessment, which may have limited the accuracy of periodontal classification. The control group consisted of patients presenting to the clinic for the first time. In all patients, periodontal tissue status was routinely assessed by measuring PPD and (clinical attachment level) CAL. However, due to the inability to obtain reliable CAL measurements in the study group, only the PPD index was used for comparative analysis between the groups. The authors are aware that tests performed in hospital settings, such as mirror tests, mSBI, and API, are simplified; thus, the results might be less accurate. Further studies are needed to determine whether patients reported that dryness was merely a subjective sensation or whether their salivation was impaired.
Second, xerostomia was assessed using a simple clinical test and patient self-report, without the use of validated questionnaires or objective salivary flow measurements, which limits the ability to distinguish subjective dryness from true hyposalivation.
Third, the study was conducted in a single center, which may limit the generalizability of the findings.
Fourth, due to incomplete availability of sociodemographic data, baseline comparisons were performed on a subset of the control group, which may reduce the precision of group comparability assessment.
Finally, the cross-sectional design and the lack of multivariable analyses limit the ability to draw causal conclusions and to fully control for potential confounders such as age, education level, and socioeconomic factors.
This study did not confirm any links between periodontal disease and MS.
The incidence of periodontitis in the MS group was lower than that in the control group, probably because of greater motivation in the MS patient group. Poorer hygiene, heavier gingival bleeding, and fewer teeth were related to greater disability. Symptoms of xerostomia were most common in older patients treated with IFN.
Research concept and design: SK-S, MT, and MR; Supervising the project: MLW; Acquisition of data: SK-S, MT, and MR; Data analysis and interpretation: SK-S, MT, and MR; Writing – Original draft preparation: SK-S, MT, and MR; Writing – Review and editing: RK and MLW; Visualization: SK-S, MT, and MR; Literature review: SK-S, MT, and MR; Final proofreading and approval of the version for publication: RK and MLW.
Sylwia Klewin-Steinböck https://orcid.org/0000-0001-7988-1282
Mateusz Tarnowski https://orcid.org/0000-0002-1060-7581
Maciej Raczkowski https://orcid.org/0000-0002-6144-3556
Radosław Kaźmierski https://orcid.org/0000-0002-9760-4884
Marzena Liliana Wyganowska https://orcid.org/0000-0003-2029-2277
The authors have no potential conflict of interests to declare.
This study was conducted in accordance with established ethical standards and guidelines for scientific research. Prior to the commencement of the study, ethical approval was obtained from the appropriate institutional ethics committee (Resolution No. 1300/18, 06.12.2018). All procedures involving human participants were performed in compliance with the principles outlined in the Declaration of Helsinki and relevant national regulations.
Informed consent was obtained from all individual participants included in the study. Participation was voluntary, and participants were informed of their right to withdraw at any stage without any consequences. All data were collected and processed anonymously to ensure confidentiality and privacy.
The application includes a copy of the approvals from the bioethics committee.