
Vitreomacular traction (VMT) syndrome occurs when posterior vitreous detachment (PVD) induces traction on the macula. This traction can lead to the development of intraretinal pseudocysts, detachment of the fovea from the retinal pigment epithelium (RPE), or a combination of both, resulting in distortion or deterioration of sight [1]. Several factors contribute to traction during PVD. VMT could be isolated or associated with other macular abnormalities such as age-related macular degeneration (AMD), retinal vein occlusion (RVO), and diabetic retinopathy (DR). However, recent studies increasingly highlight a strong connection between VMT and DR. The Relationship between these two conditions is strong enough that screening for VMT using optical coherence tomography (OCT) is recommended when evaluating patients with DR [2]. In DR, the thickened posterior hyaloid membrane of the vitreous becomes infiltrated with glial and epithelial cells, similar to what is observed in idiopathic or non-diabetic VMT.
The contraction of these migrating cells increases vitreomacular adhesion strength and tension on the detached posterior hyaloid membrane. Additionally, intraocular inflammation associated with DR, which is caused by the presence of cytokines and vascular endothelial growth factors (VEGF) in the vitreous, can result in even stronger vitreomacular adhesion and traction compared to idiopathic VMT [3, 4]. VMT is estimated to affect approximately 22.5 individuals per 100,000 and is associated with other retinal disorders such as cystoid macular edema, age-related macular degeneration, macular telangiectasia, retinal vein occlusion, and intraocular tumors [5]. Branch retinal vein occlusion (BRVO) occurs at arteriovenous crossing sites, where the vein and artery share a common adventitial sheath [6].
At these locations, arterial compression of the vein can lead to the formation of a blood clot [7]. A similar process can occur in VMT, where the attachment of the posterior hyaloid membrane to the retina near blood vessels may also trigger clot formation [8].
In most cases, eyes affected by VMT continue to worsen, resulting in a decline in VA. While spontaneous detachment of the vitreous can stop the progression and maintain vision at a stable level, this happens relatively rarely [9]. Patients who undergo surgical intervention generally achieve significantly better visual outcomes [10]. This article describes the case of a patient admitted to the Department of Ophthalmology at UCK in Katowice, Poland, presenting with severe vitreoretinal traction syndrome complicated by diabetic retinopathy and branch retinal vein occlusion.

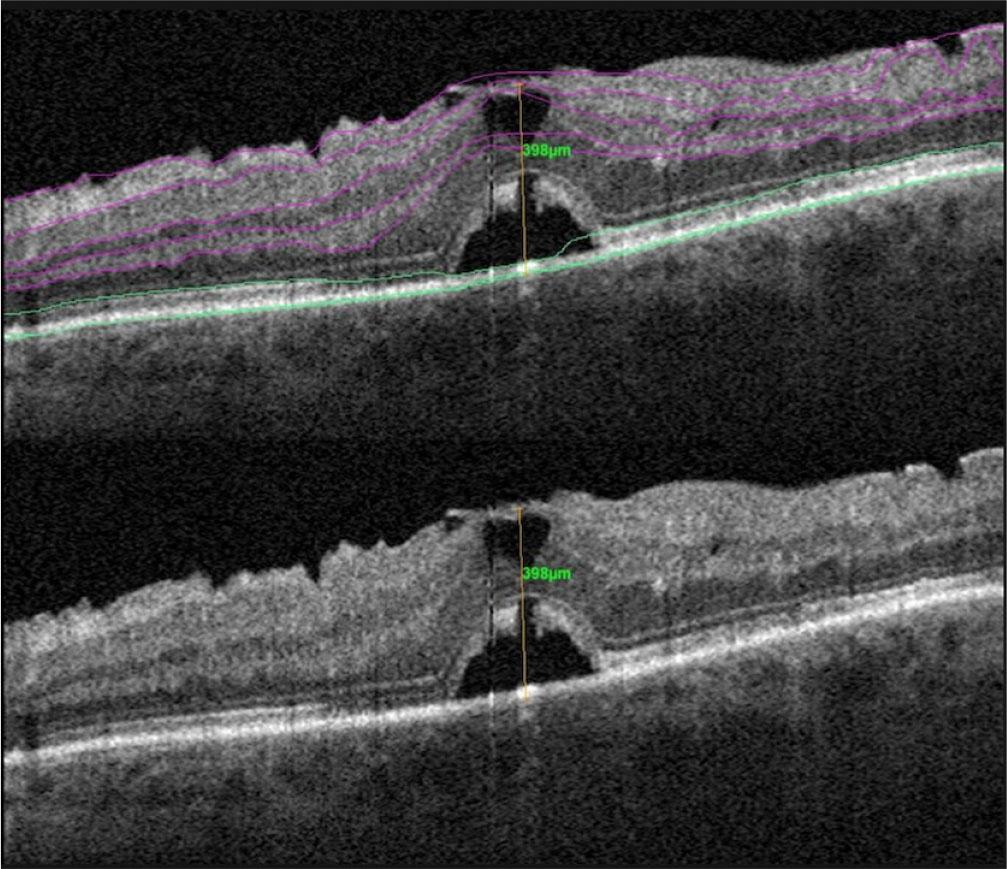
OCT scan of the left eye, taken using Carl Zeiss Meditec
A 69-year-old patient reported to the Ophthalmology Clinic due to a decline in his vision in the left eye. His medical history included a 30-year duration of diabetes, on insulin therapy for the past 5 years. The patient also has a complicated cortical-nuclear cataract in the right eye (RE) and pseudophakia in the left eye (LE). The medical history includes previous retinal laser treatments for DR in both eyes and an episode of BRVO in the LE, which occurred 6 months before the patient presented to the Ophthalmology Clinic. Additionally, there are signs of DR and diabetic macular edema (DME) in both eyes, with a predominance in the LE. On admission, the patient’s visual acuity (VA) was 0.02 in the left eye and 1.0 in the right eye, measured using the Snellen scale. Intraocular pressure (IOP) was measured at 20 mmHg in both eyes.
The left eye’s OCT revealed VMT, with an elevation of 961 μm, and a vitreomacular adhesion, with an attachment size of 427 μm. Signs of intraretinal edema were also detected.
After evaluation and additional diagnostic tests, the patient was qualified for 25G pars plana vitrectomy (PPV). Local anesthesia was administered through a peribulbar injection using a mix of 2% lignocaine and 0.5% bupivacaine solution in a 1:1 ratio. Three trocars were inserted at approximately 5, 2, and 10 o’clock positions. A 1,2 mm nasal incision in the clear cornea close to the limbus (Fig. 3-A) was used to inject Mydrane into the anterior chamber. This solution contained 0.2 mg tropicamide, 3.1 mg phenylephrine, and 10 mg lidocaine per 1 ml. Infusion was connected in the inferotemporal quadrant. During the attempt to detach the posterior hyaloid membrane, exceptionally strong adhesion was observed in the macular area (Fig. 3-B). The vitreous in this region was partially removed mechanically using ILM forceps and partially with a vitrectome. Brilliant blue G dye was applied for membrane visualization (Fig. 3-C). Both the epiretinal membrane (ERM) and the internal limiting membrane (ILM) were removed (Fig. 3-D-F). A fluid-air exchange was performed, followed by an air-25% SF6 gas exchange. Postoperatively, the patient was instructed to maintain a face-down head position.

OCT scan of the left eyek taken using an Optovue SOLIX

Vitrectomy intraoperative images
The surgery went well, without any complications. After 38 days, OCT imaging of the LE showed a release of macular traction and improvements in the structural morphology of the operated area, including the beginning of subretinal fluid resorption (Fig. 4).
OCT scan of the left eye, taken using the Optovue AngioVue
Ten days after the procedure, a follow-up examination showed that VA in the LE had improved to 0.3, with IOP at 16 mmHg. At the 38-day follow-up, the VA in the LE remained stable.
Vitreomacular interface (VMI) disorders can lead to various macular conditions, such as vitreomacular adhesion (VMA), VMT, and full-thickness macular hole (FTMH). Typically, during the early decades of life, the vitreous gel adheres completely to the ILM, with the vitreous body fully attached to the entire retina surface. Around the age of 40, the vitreous body starts undergoing structural changes, leading to either a complete or incomplete PVD. In incomplete PVD, the vitreous gel liquefies without a simultaneous weakening of its attachment to the retina. The location where these disorders occur depends on areas where the vitreous attachment to the retina is strongest and where the gel is most liquefied [11]. According to OCT classification, VMA represents the initial stage of incomplete PVD, characterized by elevation of the posterior vitreous cortex above the retinal surface while maintaining attachment within a radius of approximately 3 mm around the fovea. The next stage, VMT, is identified using OCT B-scans involve perifoveal PVD accompanied by specific anatomical changes: perifoveal detachment of the vitreous cortex, continued attachment of the vitreous cortex within 3 mm of the fovea, distortion of the foveal surface, structural changes within the retina, and elevation of the fovea above the RPE. If these retinal changes progress further and result in a breakthrough, all retinal layers from the ILM to the RPE, visible in at least one OCT B-scan, it is defined as an FTMH [1].
The development of VMT in DR follows a different pathophysiological mechanism compared to VMT resulting from non-diabetic etiologies [3]. In patients with DR, the metabolic activity in the vitreous shows significantly altered glucose metabolism compared to individuals without diabetes. There is a distinct decrease in glycolysis-related metabolites, accompanied by a tenfold increase in pentose phosphate pathway products [12]. The increased activity of the pentose phosphate pathway is observed under oxidative stress induced by diabetes and plays a protective role [13]. Advanced glycation end products present in the vitreous of eyes with DR cause hyaluronic acid degradation and liquefaction of the vitreous, leading to vitreoschisis or incomplete PVD [3, 14]. Additionally, differences in the levels of aspartate and linoleic acid have been observed depending on the severity of DR. Progression to proliferative diabetic retinopathy (PDR) is associated with a decrease in linoleic acid levels and an increase in aspartate levels [15]. In DR, changes are not limited to vitreous metabolism. Connective tissue growth factors (CTGF), present even in the preclinical stages of the disease, contribute to fibrotic responses [16]. Diabetes affects the vitreous and changes the ILM, which thickens due to excess fibronectin and various collagens. Eyes with DR also show increased levels of extracellular matrix proteins. These combined factors lead to much stronger adhesion between the vitreous and the macula, intensifying vitreomacular traction [3]. This adhesion is so strong that uncomplicated PVD occurs significantly later in eyes with DR than in healthy individuals [17].
BRVO commonly occurs at arteriovenous crossing sites, where the vein and artery share a common adventitial sheath [6]. At these locations, arterial compression of the vein can lead to loss of venous endothelial cells, creating turbulent blood flow and formation of a blood clot, eventually resulting in a blockage [7]. A similar process can occur in VMT when the posterior hyaloid membrane attaches to the retina near blood vessels. This adhesion can deform the retinal veins, causing turbulent blood flow, increasing the risk of clot formation and vein occlusion. Up to 25% of VMT cases are associated with diffuse perivascular edema in the affected section of the vessel [8].
DME is the leading cause of vision loss in patients with DR [18]. The accumulation of fluid in the macular area leads to secondary retinal swelling, referred to as DME, which can occur at any stage of DR but becomes more common as the disease progresses [19]. This fluid buildup is primarily associated with a breach in the retinal barrier, a process in which VEGF plays a critical role [20]. Unfortunately, up to 30% of patients do not respond to intravitreal anti-VEGF treatments [21]. In cases of tractional DME, vitrectomy with ILM and ERM removal often proves effective and should be considered an early treatment option [4].
Cystoid macular edema (CME) is a condition in which fluid accumulates beneath the retina in the macular area due to damage to the blood-retinal barrier. CME risk factors can be divided into inflammatory, vascular, and postoperative categories. Inflammatory factors include conditions such as uveitis, pars planitis, and human immunodeficiency virus (HIV) infection. Vascular factors mainly involve diabetic macular edema resulting from retinopathy and retinal vein occlusion [22]. Since our patient had both diabetic macular edema and BRVO and had also undergone surgery, we cannot determine which of these factors specifically led to the accumulation of subretinal fluid.
Wilson DS et al. treated a patient with VMT and an initial VA of 0.28 using PPV. The procedure involved removing ILM and ERM, followed by SF6 gas endotamponade. However, eight months after surgery, the patient’s VA decreased to 0.125, with subfoveal subretinal fluid (SRF) detected on spectral domain-OCT (SD-OCT) as a postoperative complication [23]. Kumar N et al. performed PPV on a patient with VMT, intraretinal cysts, and RPE detachment. The ILM was removed during the surgery, followed by a fluid-air exchange and SF6 gas endotamponade. At three months postoperatively, OCT imaging showed resolution of the partial-thickness macular hole, intraretinal cysts, and RPE detachment. The patient’s VA improved to 0.5 at three months and 0.66 six months after the surgery [24]. Tayyab M et al. described a patient with VA limited to counting fingers and an SD-OCT showing a Grade 1b macular hole with focal VMT. The initial surgery involved PPV with ILM removal and air endotamponade. However, 10 days after the procedure, OCT revealed an FTMH with rolled edges, and the patient’s VA remained at the level of hand movements. A decision was made to reoperate. During the second procedure, PPV was performed again, with additional ILM peeling, staining with brilliant peel dye, and 14% C3F8 gas endotamponade. Six weeks after the reoperation, the patient’s VA improved to 0.17, and OCT confirmed the restoration of normal foveal anatomy [25].
These cases highlight the importance of ILM removal as a key step in PPV for VMT, ensuring the best possible postoperative outcomes. In our clinical case, the ILM and ERM were also removed. The use of gas endotamponade, rather than air, proved to be essential, too. As seen in the case, Tayyab M et al. reported that combining ILM peeling with gas endotamponade significantly improved the patient’s VA after an earlier attempt with air endotamponade had failed. SF6 gas was used in our case, which is consistent with similar studies [23, 24, 25]. Proper management, combined with precise and careful surgical technique, improved the patient’s VA from 0.02 to 0.6 just 38 days after the procedure.
The literature describes several approaches to managing VMT. Aside from surgery (vitrectomy), alternative strategies include watchful waiting or pharmacological vitreolysis with ocriplasmin [26]. Without treatment, VMT rarely resolves spontaneously by releasing VMA, and patients typically face the risk of further visual deterioration. Ocriplasmin is an enzyme administered through injections directly into the vitreous cavity to reduce VMA, thereby treating VMT and macular holes [27]. It breaks down collagen, fibronectin, and laminin, causing the vitreous gel to liquefy and reducing its attachment to the retina [28]. Successful anatomical outcomes with ocriplasmin, observed within 28 days, have decreased the need for surgical intervention, PPV, and lowered treatment costs [27]. However, this medication does have certain limitations. A study by Jackson et al. indicated that the effectiveness of ocriplasmin was lower in patients with coexisting ERM, broad VMA (>1500 μm), DR, or pseudophakia [29]. Given the numerous ocular conditions present in our patient, we ultimately decided to proceed with surgical treatment.
A key limitation of this study is that it involves only one patient, which means we cannot perform statistical analysis or generalize our findings to a broader population. In the future, we plan to expand this research to include more patients, allowing us to better understand and apply these results in clinical practice. However, our case report presents high-quality intraoperative images, making it a valuable educational example of a patient with more than one factor contributing to vitreomacular traction, including DR and BRVO.
Despite the strong vitreoretinal adhesion caused by coexisting retinal diseases, 25G PPV with ERM and ILM peeling, combined with brilliant blue G staining, is an effective treatment for vitreomacular traction syndrome complicated by diabetic retinopathy and branch retinal vein occlusion. This method helps restore useful visual acuity and improve the patient’s quality of vision.