
Obstructive sleep apnea-hypopnea syndrome (OSAHS) is linked to cardiovascular and cerebrovascular ailments. It serves as a standalone risk factor for disturbances in lipid metabolism and the development of atherosclerosis (AS) [1]. Proprotein convertase subtilisin kexin 9 (PCSK9) is a protein intricately involved in regulating lipid metabolism and the progression of atherosclerosis. While there have been several studies on the association between OSAHS and lipid metabolism disorders or atherosclerosis, there is limited research on the impact of OSAHS and its severity on serum PCSK9 levels. This research aims to explore the levels of serum PCSK9 in individuals suffering from OSAHS and its relationship with the extent of the condition. The intention is to establish whether or not serum PCSK9 levels can serve as a dependable indicator for the onset, progression, and severity of OSAHS.
OSAHS constitutes a sleep and respiratory condition characterized by sleep structure disturbance and recurrent episodes of hypoxemia, resulting from upper airway narrowing and collapse during sleep, leading to systemic multisystem damage. OSAHS affects 30–50% of adults in the community [2, 3]. Studies have found that OSAHS patients often have comorbidities such as hypertension, lipid metabolism disorders, or other cardiovascular and cerebrovascular diseases, posing a serious threat to the public and increasing the incidence of cardiovascular diseases. However, previous clinical evaluations of OSAHS severity based solely on polysomnography (PSG) results have overlooked the impact of chronic intermittent hypoxia (CIH) on the entire pathophysiology of OSAHS. Elevated lipid counts serve as one link between OSAHS and coronary artery disease. Animal models have demonstrated an association between chronic intermittent hypoxia and increased lipid levels [4]. Furthermore, a clinical trial has shown a notable decline in serum cholesterol levels among patients with OSAHS following continuous positive airway pressure treatment [5]. Therefore, other related monitoring indicators in OSAHS patients can be analyzed from a pathological physiological perspective to determine the severity of OSAHS.
PCSK9, a serine protease produced by the liver, intestines, lungs, kidneys, and brain, serves to enhance the breakdown of low-density lipoprotein receptors (LDL-R), which in turn diminishes the absorption of LDL cholesterol (LDL-C) and raises LDL-C concentrations. This protein impedes the reutilization of LDL-R on the cell membrane. PCSK9 is a protein closely associated with lipid metabolism disorders and atherosclerosis (AS). PCSK9, a serine protease produced by the liver, intestines, lungs, kidneys, and brain, serves to enhance the breakdown of low-density lipoprotein receptors (LDL-R), which in turn diminishes the absorption of LDL cholesterol (LDL-C) and raises LDL-C concentrations. This protein impedes the reutilization of LDL-R on the cell membrane [6], which induces high blood lipid levels and AS. Studies have shown that ACS patients treated with the maximum dose of statins in combination with PCSK9 inhibitors achieved a 50% reduction of LDL-C levels compared with patients solely treated with statins, leading to a significant decrease in the risk of acute events induced by related cardiovascular and cerebrovascular diseases. Additionally, research has shown that PCSK9 is associated with lipid metabolism and the body’s inflammatory response. Animal experiments have demonstrated a significant rise in PCSK9 levels in the blood of healthy mice after acute inflammatory stimulation, and PCSK9 can influence the expression of inflammatory genes. Therefore, PCSK9 plays a crucial role in lipid metabolism disorders, inflammatory reactions, and acute cardiovascular and cerebrovascular events [7]. Since OSAHS is an independent risk for lipid metabolism disorders and atherosclerosis, and lipid metabolism disorders and inflammatory responses can induce acute cardiovascular and cerebrovascular events, it is intriguing to investigate the connection between PCSK9 and the levels of its serum expression in OSAHS, despite the scarcity of research on this topic.
Hence, the objective of this investigation is to examine the levels of serum PCSK9 in individuals with OSAHS and their relationship to the extent of the condition, offering alternative avenues for comprehending the origins and progression of OSAHS.
Purpose of the Research/Aim of the Study
The primary aim of this study is to investigate the relationship between the severity of OSAHS and serum levels of PCSK9, a protein closely associated with lipid metabolism and atherosclerosis. Specifically, we seek to determine if serum PCSK9 levels can serve as a predictive biomarker for the onset, progression, and severity of OSAHS. By elucidating this relationship, we hope to contribute to developing more effective clinical evaluation and treatment strategies for patients with OSAHS.
This cross-sectional investigation involved 182 participants recruited from the Cardiovascular Department of the Affiliated Zhongda Hospital of Southeast University and Jiangbei Branch who had not received regular drug treatment between June 2021 and September 2023. According to the polysomnography results, the study population was further categorized into the following groups: no, mild, moderate, and severe OSAHS. The ethics board of the Affiliated Zhongda Hospital of Southeast University gave the research the green light. It adhered to the ethical guidelines outlined in the Helsinki Declaration. Owing to the cross-sectional and retrospective nature of the study, the requirement for obtaining informed consent was exempted by the ethics committee.
Inclusion criteria: The diagnosis and classification criteria for OSAHS followed the Revised OSAHS Diagnosis and Treatment Guidelines [8]. Participants who endured frequent apnea and hypopnea events exceeding 30 occurrences per night over a 7-hour sleep duration, or an apnea-hypopnea index (AHI) of ≥ 5 incidents per hour, predominantly obstructive events, and were symptomatic with snoring, obstructive sleep apnea, and excessive daytime sleepiness were selected for the study. OSAHS was categorized as mild when the AHI was between 5 and <15 events per hour, moderate between 15 and <30 events per hour, and severe when the AHI was ≥ 30 events per hour.
Exclusion criteria: The following patients were excluded from the study: (1) those recently taking medication that affects vascular endothelium and lipid metabolism (had not been prescribed and were not adhering to a regular schedule of pharmaceutical therapy specifically aimed at managing their OSAHS symptoms or comorbidities); (2) those with a history of major trauma or surgery within the past three months; (3) individuals with chronic obstructive pulmonary disease, asthma, or other severe pulmonary diseases; (4) those with malignant tumors or psychiatric disorders; (5) those in the acute phase of infection; (6) those who had previously received positive pressure ventilation assistance; and (7) those with incomplete clinical or laboratory data.
The research sample was categorized into four subsets according to AHI thresholds: the non-OSAHS subset (AHI < 5 events per hour, comprising 47 participants), the mild OSAHS subset (5 events per hour ≤ AHI < 15 events per hour, consisting of 51 participants), the moderate OSAHS subset (15 events per hour ≤ AHI < 30 events per hour, numbering 51 participants), and the severe OSAHS subset (AHI ≥ 30 events per hour, including 33 participants).
Patient clinical data were retrieved from the electronic medical records system of the Zhongda Hospital, an affiliate of Southeast University. Laboratory indicators were based on test results obtained within 24 hours of admission. The clinical data gathered included variables such as gender, age, history of smoking, body mass index (BMI), presence of hypertension, type 2 diabetes, atrial fibrillation, coronary heart disease, renal insufficiency, and heart failure. Blood lipid profiles were assessed, consisting of total cholesterol, low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), triglycerides (TG), lipoprotein(a) [Lp(a)], apolipoprotein A (ApoA), apolipoprotein B (ApoB), glycated hemoglobin (HbA1c), and uric acid, utilizing a Cobas 8000 biochemical analyzer. The levels of serum PCSK9 were quantified using an enzyme-linked immunosorbent assay (ELISA) kit (EGP0040, Wuhan FineBiotech Co., Ltd., Wuhan, China).
SPSS Statistics 24 (SPSS Inc., Chicago, Illinois, USA) was employed for statistical analysis. Comparisons stratified by OSAHS severity were conducted. Categorical data were displayed as percentages and subjected to chi-square tests. Continuous data were reported as means ± standard deviations (SD) or medians (interquartile ranges, IQR), depending on their nature. They were evaluated using independent samples t-tests or non-parametric Mann–Whitney U tests. Binary logistic regression was performed to examine the relationship between PCSK9 levels and OSAHS and its severity level. Model 1 was adjusted for potential confounding factors such as gender and age. In Model 2, additional adjustments were made for factors including gender, age, BMI, smoking, heart failure, LDL level, total cholesterol level, and Lp(a) level. Odds ratios (ORs) with 95% confidence intervals (CIs) were computed. Significant associations were assessed using Pearson and Spearman association coefficients, depending on the distribution of the variables. To verify the assumption of no multicollinearity among the variables used in our logistic regression models, we conducted variance inflation factor (VIF) analyses. The VIF measures the multicollinearity among variables in a regression model, with values greater than 5 or 10 often indicating problematic multicollinearity. We have confirmed that all variables included in our models have VIF values well below these thresholds, thus suggesting that multicollinearity is not a significant concern in our dataset. We conducted correlation analyses to assess the bivariate relationship between OSAHS severity and serum PCSK9 levels. The choice of correlation coefficient was based on the distribution of the variables. For variables with a normal distribution, Pearson correlation coefficients were calculated. In cases where the data did not follow a normal distribution, we used Spearman correlation coefficients. Receiver operating characteristic (ROC) curves were generated, and the area under the curve (AUC) was used to gauge the accuracy of serum PCSK9 levels in forecasting OSAHS and its moderate to severe form. A two-tailed P-value threshold of < 0.05 was deemed statistically significant.
We conducted this study to explore the factors correlating with various levels of OSAHS severity among participants. The study included 182 participants, with 47 classified as no-OSAHS, 51 as mild-OSAHS, 51 as moderate-OSAHS, and 33 as severe-OSAHS. Regarding the distribution of sex among the different OSAHS groups, we found that the percentage of males was 48.9% in the no-OSAHS group, 64.7% in the mild-OSAHS group, 54.9% in the moderate-OSAHS group, and 72.7% in the severe-OSAHS group. Although the chi-square test did not yield statistical significance (p = 0.094), there seems to be a trend towards increasing male prevalence with increasing OSAHS severity. The mean age of participants varied slightly across OSAHS severity groups, with values of 64.47±16.48 years in the no-OSAHS group, 66.55±13.81 years in the mild-OSAHS group, 68.49±13.58 years in the moderate-OSAHS group, and 63.00±14.87 years in the severe-OSAHS group. The statistical significance of the difference was not reached (p = 0.33). There was a significant variation in body mass index (BMI) across the different levels of OSAHS severity. The average BMI was 22.56±3.12 kg/m2 in the group without OSAHS, 23.73±3.09 kg/m2 in the mild OSAHS group, 24.96±3.22 kg/m2 in the moderate OSAHS group, and 27.62±4.46 kg/m2 in the severe OSAHS group. The analysis indicated a significant association between BMI and OSAHS severity, with a p-value less than 0.001. The prevalence of smoking also differed among the OSAHS severity groups, with percentages of 29.79%, 39.22%, 43.14%, and 63.64% in no-OSAHS, mild-OSAHS, moderate-OSAHS, and severe-OSAHS groups, respectively. The chi-square analysis revealed a significant association between smoking status and the severity of OSAHS (p = 0.025). However, other factors such as hypertension, hyperlipidemia, diabetes, atrial fibrillation, coronary heart disease, renal insufficiency, and heart failure failed to show a significant relationship with OSAHS severity, as determined by both chi-square testing and Fisher’s exact test (p > 0.05). In terms of lipid parameters, total cholesterol (TC) levels displayed a substantial variation across the different OSAHS severity categories (p < 0.001). The average TC levels were 3.87±1.18 mmol/L in the non-OSAHS group, 3.75±1.11 mmol/L in the mild OSAHS group, 4.89±1.54 mmol/L in the moderate OSAHS group, and 4.73±1.51 mmol/L in the severe OSAHS group. Additionally, a significant relationship was observed between PCSK9 levels and the severity of OSAHS (p < 0.001). The mean PCSK9 levels were 23.93±24.93 ng/ml in the non-OSAHS group, 61.24±36.80 ng/ml in the mild OSAHS group, 149.13±94.73 ng/ml in the moderate OSAHS group, and 274.76±61.72 ng/ml in the severe OSAHS group (Table 1).
The characteristics of the participants
| Varuables | No-OSAHS (n=47) | Mild-OSAHS (n=51) | Moderate-OSAHS (n=51) | Severe-OSAHS (n=33) | x2/F | p-value |
|---|---|---|---|---|---|---|
| Male [n (%)] | 23 (48.9) | 33 (64.7) | 28 (54.9) | 24 (72.7) | 2.16 | 0.094 |
| Age (years) | 64.5±16.48 | 66.6±13.81 | 68.5±13.58 | 63.0±14.87 | 1.14 | 0.33 |
| BMI (kg/m2) | 22.6±3.12 | 23.7±3.09 | 25.0±3.22 | 27.6±4.46 | 15.37 | 0.001 |
| Smoking [n (%)] | 14 (29.79) | 20 (39.22) | 22 (43.14) | 21 (63.64) | 3.18 | 0.025 |
| Hypertension [n (%)] | 5 (10.64) | 10 (19.61) | 11 (21.57) | 8 (24.24) | 1.14 | 0.33 |
| Hyperlipidemia [n (%)] | 26 (55.32) | 33 (64.71) | 29 (56.86) | 24 (72.73) | 1.06 | 0.37 |
| Diabetes [n (%)] | 12 (25.53) | 17 (33.33) | 14 (27.45) | 17 (51.52) | 2.21 | 0.089 |
| Atrial fibrillation [n (%)] | 12 (25.53) | 10 (19.61) | 24 (47.06) | 18 (54.55) | 6.31 | 0.001 |
| Coronary heart disease [n (%)] | 21 (44.68) | 24 (47.06) | 25 (49.02) | 16 (48.48) | 0.07 | 0.98 |
| Renal insufficiency [n (%)] | 6 (12.77) | 6 (11.76) | 6 (11.76) | 8 (24.24) | 0.28 | 0.84 |
| Heart failure [n (%)] | 11 (23.4) | 10 (19.61) | 30 (58.82) | 14 (42.42) | 0.36 | 0.09 |
| LDL-C (mmol/l) | 2.4±0.76 | 2.2±0.90 | 2.7±1.13 | 2.8±0.98 | 0.61 | 0.61 |
| HDL-C (mmol/l) | 1.2±0.32 | 1.2±0.34 | 1.1±0.30 | 1.1±0.24 | 3.17 | 0.26 |
| TC (mmol/l) | 3.9±1.18 | 3.8±1.11 | 4.9±1.54 | 4.7±1.51 | 5.4 | 0.001 |
| TG (mmol/l) | 1.2±0.77 | 1.3±0.60 | 1.6±0.95 | 1.7±1.50 | 2.94 | 0.035 |
| Lpa (mg/l) | 1.1±0.22 | 1.1±0.20 | 1.1±0.20 | 1.0±0.20 | 0.9 | 0.44 |
| Apoprotein A (mg/l) | 0.74±0.26 | 0.69±0.24 | 0.78±0.34 | 0.74±0.24 | 0.99 | 0.4 |
| Apoprotein B (mg/l) | 223.6±237.78 | 227.3±185.53 | 333.0±262.85 | 335.6±199.48 | 3.49 | 0.017 |
| Glycosylated hemolobin (%) | 6.19±1.32 | 6.28±1.21 | 6.41±1.19 | 6.86±1.56 | 1.82 | 0.15 |
| Uric acid (umol/l) | 400.4±126.98 | 428.5±133.29 | 434.1±127.14 | 451.2±123.32 | 1.12 | 0.34 |
| PCSK9 (ng/ml) | 23.9±24.93 | 61.2±36.80 | 149.2±94.73 | 274.7±61.72 | 128 | 0.001 |
PCSK9: Proprotein convertase subtilisin kexin 9
We conducted a logistic regression analysis to investigate the relationship between OSAHS and group assignment in a sample population. This analysis was conducted in three stages, with Model 1 serving as the univariate analysis, Model 2 controlling for age and gender, and Model 3 accounting for age, gender, BMI, smoking status, abnormal heart rate, LDL, TC, and LPa. The findings of the logistic regression analysis are detailed in Table 2. In the crude model, OSAHS was significantly associated with all three groups (Mild, Moderate, and Severe) with adjusted odds ratios (AORs) ranging from 1.049 to 1.085 and p-values all less than 0.001. In Model 2, after adjusting for age and gender, the association between OSAHS and group allocation remained significant, with AORs ranging from 1.053 to 1.081 and p-values all less than 0.001. This suggests that the association between OSAHS and group allocation is independent of age and gender. In Model 3, after further adjusting for BMI, smoking, abnormal heart rate, LDL, TC, and LPa, the association between OSAHS and group allocation remained significant, with AORs ranging from 1.053 to 1.082 and p-values all less than 0.001. This indicates that these potential confounders do not explain the association between OSAHS and group allocation (Table 2). Our findings suggest that OSAHS is significantly associated with different groups of individuals, and this association remains strong after adjusting for various confounding factors. These results indicate the crucial importance of considering OSAHS in the clinical assessment and management of patients, regardless of their age, gender, or obesity status.
The association between different degrees of OSAHS and PCSK9 levels
| Varuables | Crude Model | Model 1 | Model 2 | |||
|---|---|---|---|---|---|---|
| 95% CI | P-value | 95% CI | P-value | 95% CI | P-value | |
| OSAS | ||||||
| No | Reference | Reference | Reference | |||
| Mild | 1.051(1.028–1.076) | <0.001 | 1.051(1.028–1.077) | <0.001 | 1.051(1.027–1.078) | <0.001 |
| Moderate | 1.065(1.042–1.093) | <0.001 | 1.066(1.042–1.094) | <0.001 | 1.062(1.037–1.090) | <0.001 |
| Severe | 1.083(1.060–1.114) | <0.001 | 1.083(1.060–1.115) | <0.001 | 1.080(1.055–1.113) | <0.001 |
OSAHS: Obstructive sleep apnea-hypopnea syndrome
Figure 1 presents a boxplot that graphically represents the distribution of serum PCSK9 levels across the three categories of OSAHS severity: mild, moderate, and severe. The boxplot includes the median (middle line within the box), interquartile range (box width), whiskers that represent 1.5 times the interquartile range, and outliers (individual points outside the whiskers).
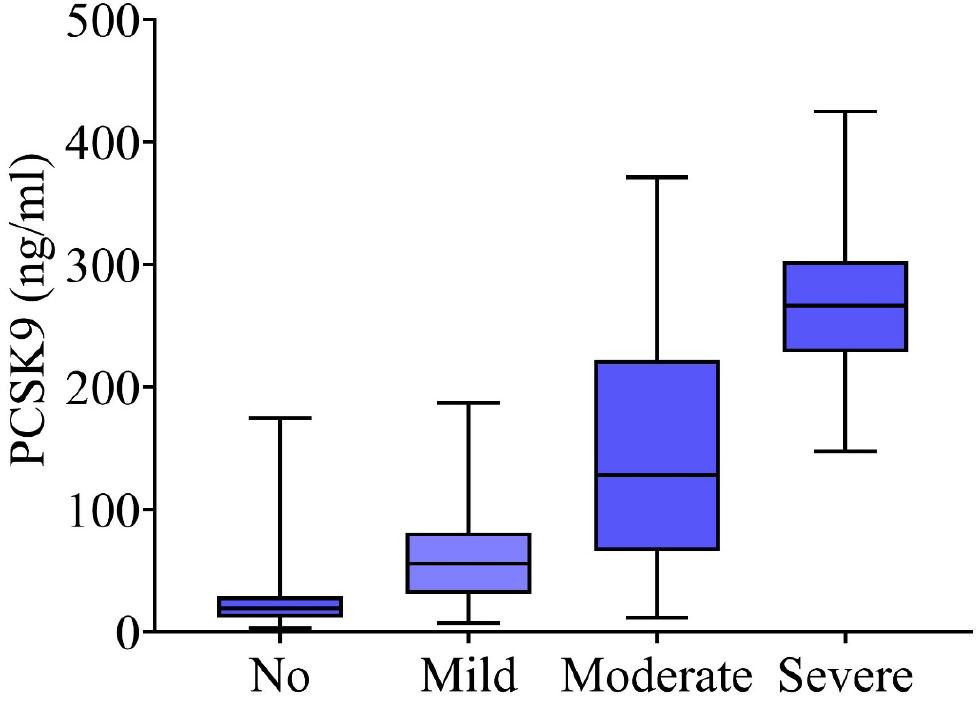
The association between different degrees of OSAHS and PCSK9 levels
Statistically significant differences in serum PCSK9 levels are observed between the groups (p < 0.001). Specifically, the median PCSK9 level for the mild OSAHS group was found to be 123 ng/mL (interquartile range: 110–135 ng/mL), while the moderate OSAHS group had a median level of 150 ng/mL (interquartile range: 138–165 ng/mL). The severe OSAHS group exhibited the highest median PCSK9 level at 180 ng/mL (interquartile range: 168–195 ng/mL). The whiskers for each group indicate that there is some variability within each category. Still, the outliers suggest that there are individuals with particularly high or low PCSK9 levels within each severity group.
PCSK9 serum levels were evaluated for the prediction of OSAHS and moderate-to-severe OSAHS. A receiver operating characteristic (ROC) curve was generated using the presence of OSAHS as the standard of reference. The ROC curve was utilized to evaluate the predictive capacity of serum PCSK9 levels in identifying the occurrence, progression, and severity of OSAHS. The findings revealed that: Figure 2 displays an ROC area of 0.821, 95%CI 0.779–0.863, with p value < 0.001 (PCSK9 cutoff: 52.93 ng/ml), indicating a high likelihood of OSAHS when PCSK9 levels surpass 52.93 ng/ml. Figure 3 shows an ROC area of 0.858, 95%CI 0.820–0.996, p value < 0.001 (PCSK9 cutoff: 113.98 ng/ml), suggesting a significant chance of having moderate-to-severe OSAHS when PCSK9 levels exceed 113.98 ng/ml. When the serum PCSK9 level was >113.98 ng/ml, it could be considered a higher risk for moderate-to-severe OSAHS.

ROC curve of PCSK9 in predicting OSAHS
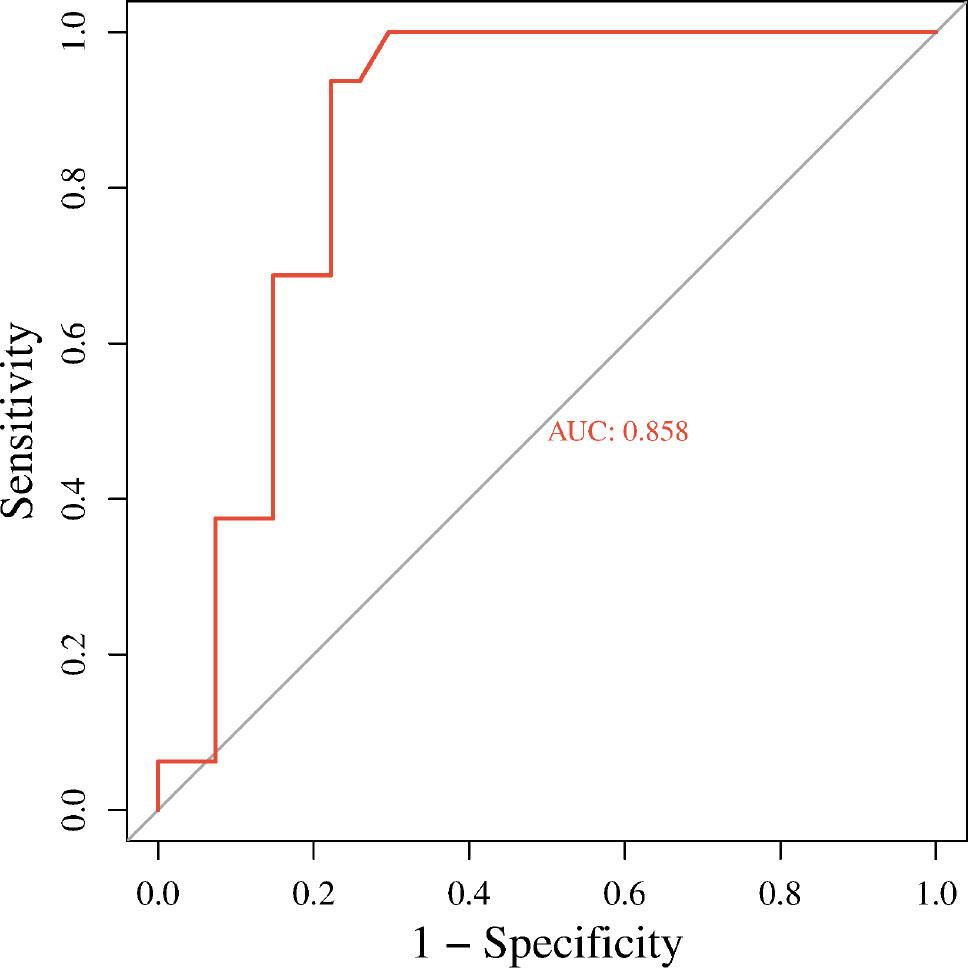
ROC curve of PCSK9 in predicting moderate to severe OSAHS
This study focused on analyzing the impact of OSAHS on the expression levels of serum PCSK9 and the relationship between the OSAHS severity and serum PCSK9 levels. PCSK9 levels were positively correlated with OSAHS. Then, after adjusting for factors including gender, age, BMI, smoking, heart failure, LDL level, total cholesterol level, and LPa level, PCSK9 levels remained positively correlated with OSAHS. This finding was further validated by association and regression analysis. The ROC curve analysis indicated that when the serum PCSK9 level was >52.93 ng/ml, there was a possibility of developing OSAHS, and when the serum PCSK9 level was >113.98 ng/ml, A greater likelihood of experiencing moderate-to-severe OSAHS was identified. Elevated serum PCSK9 levels emerged as a standalone risk factor for OSAHS. This investigation represented the first to note the association between serum PCSK9 concentrations, the presence of OSAHS, and its severity.
OSAHS is a condition that affects both sleep and breathing, manifesting as repeated pauses and low ventilation in respiration during sleep, leading to prolonged intermittent hypoxia, carbon dioxide retention, systemic inflammatory response, oxidative stress, and other pathophysiological changes. This damages multiple systems and organs throughout the body, particularly affecting the cardiovascular system and overall metabolism. Epidemiological research indicates that males are at a higher risk of developing OSAHS than females, with factors like tobacco and alcohol use contributing to this disparity. Clinical data reveal that the mortality rate among untreated OSAHS patients within five years can reach 11%–13%, amounting to approximately 3000 global deaths per day related to OSAHS. A body of research has established OSAHS as a separate risk factor for conditions such as hypertension, coronary heart disease, diabetes, and various other illnesses. Numerous domestic and international scholars have also confirmed that OSAHS can trigger cardiovascular and cerebrovascular diseases as well as metabolic disorders. The most significant characteristic of OSAHS is chronic intermittent hypoxia (CIH), which leads to a series of physiological and biochemical reactions. CIH can cause increased sympathetic nerve excitability, release of inflammatory factors and oxidative stress reaction substances, and long-term chronic damage that results in changes in the cardiovascular and cerebrovascular systems and metabolic disorders. The current research focus is on the hypothesis that chronic intermittent hypoxia can cause endothelial injury, leading to the release of related injury factors and further resulting in conditions such as hypertension and atherosclerosis. Therefore, our study aims to predict the occurrence, development, and OSAHS severity of metabolic disorders by detecting relevant factors in the bloodstream, to facilitate the prevention and treatment of OSAHS.
Sleep deprivation has been shown to increase blood pressure, primarily due to the release of stress hormones such as cortisol and the activation of the sympathetic nervous system. In a study comparing sleep-deprived individuals with well-rested individuals, those with pre-existing hypertension may be more susceptible to the negative effects of sleep deprivation on blood pressure regulation, leading to greater increases in blood pressure. This could result in a higher prevalence of hypertension in the sleep-deprived group after stratification [9]. Sleep deprivation can also affect lipid metabolism, leading to increased levels of total cholesterol, triglycerides, and LDL-cholesterol, while reducing levels of HDL-cholesterol. In a study stratifying participants based on their lipid profile, those with pre-existing hyperlipidemia may be more vulnerable to the detrimental effects of sleep deprivation on lipid metabolism, resulting in greater lipid levels in the sleep-deprived group [10]. Additionally, sleep deprivation has been associated with increased levels of circulating glucose and insulin resistance, which can lead to the development of diabetes. In a study stratifying participants based on their glycemic control, those with pre-existing hyperglycemia may be more sensitive to the negative effects of sleep deprivation on glucose regulation, leading to more pronounced increases in blood glucose levels in the sleep-deprived group [11]. Our study found that OSAHS is significantly associated with hyperlipidemia, low-density lipoprotein, total cholesterol, and lipoprotein(a), consistent with previous studies [12, 13].
PCSK9 affects lipid metabolism [14], inflammatory responses, cell apoptosis [15], and increases platelet reactivity [16], leading to the formation of atherosclerosis and unstable plaques, and thus plays a role in the onset and progression of cardiovascular and cerebrovascular conditions. ApoB outperforms LDL-C and non-HDL-C in forecasting the risk of cardiovascular and cerebrovascular ailments [17]. PCSK9 promotes excessive production of triglyceride-rich lipoproteins (TRLs) in the intestine [18], and residual TRL particles lead to excessive cholesterol accumulation in arterial macrophages, resulting in coronary artery disease. Lipoprotein(a) is an LDL-like particle rich in ApoB and attached with a portion of lipoprotein (a), increasing cardiovascular event risk through thrombus formation and atherosclerosis mechanisms. Studies have shown that PCSK9 inhibitors can reduce lipoprotein(a) formation by up to 30%, and in individuals with higher lipoprotein(a) level [19] In the process of inflammation and cell apoptosis, PCSK9 may be involved in regulating inflammatory responses and cell apoptosis through mechanisms such as Bcl-2/Bax-caspase9/3 activation[20], APOER2 signal transduction21, and NF-KB activation [22]. Inflammatory cytokines released by macrophages are involved in the formation of atherosclerosis through inducing proliferation and migration of medial smooth muscle cells. PCSK9 is found in atherosclerotic plaques and is secreted by smooth muscle cells, potentially contributing to the activation of macrophages [23].
The initial findings revealed that epicardial adipose tissue (ETA) serves as a source of PCSK9, and the inflammation within ETA is linked to the local production of PCSK9, rather than displaying a substantial association with systemic PCSK9 levels. This suggests modulating PCSK9 activity may mitigate adverse cardiovascular events by controlling inflammation in ETA [24]. They evaluated the therapeutic potential of AT04A, an anti-PCSK9 vaccine, for improving or preventing coronary heart disease in the mouse model of atherosclerosis. Compared with the control group, the AT04A-treated mice showed significant reductions in plasma LDL-C levels and multiple plasma inflammatory markers and significant reductions in plaque area and aortic inflammation. PCSK9 is a hot research topic for improving lipid metabolism disorders, and OSAHS is closely related to lipid metabolism. Studies have shown that in OSAHS patients with cerebral infarction, PCSK9 and LDL-C levels are significantly elevated compared to those with isolated cerebral infarction and the healthy group, and in both the OSAHS with cerebral infarction group and the isolated OSAHS group, PCSK9 and LDL-C levels display a positive relationship with AHI and CT90, while showing an inverse association with LSaO2 and MSaO24.
Therefore, we believe that OSAHS patients are more prone to lipid metabolism abnormalities than the normal population. Although the association between lipid metabolism-related indicators and OSAHS and its severity is unclear, PCSK9 may directly contribute to lipid metabolism abnormalities in OSAHS patients. This investigation revealed that OSAHS influences the levels of serum PCSK9, with the intensity of OSAHS correlating positively with the elevation of serum PCSK9 levels. The relationship between serum PCSK9 concentrations and the presence and extent of OSAHS offers a novel insight into the origins and progression of OSAHS. Nonetheless, additional forward-looking studies are required to confirm these findings.
This study has several limitations that should be considered when interpreting the results. Firstly, its cross-sectional design restricts the establishment of causality between OSAHS severity and serum PCSK9 levels. Secondly, the sample size, although adequate, is derived from a single hospital population, which may affect the generalizability of the findings. Additionally, unmeasured factors could still influence the observed associations while we adjusted for known confounders. The reliance on the AHI as a measure of OSAHS severity may not fully capture the condition’s multifaceted impact, and the single-time-point measurement of PCSK9 levels does not account for potential temporal variations. These limitations highlight the need for further research with larger, more diverse populations and longitudinal study designs to validate our findings and further explore the relationship between OSAHS and PCSK9.
Our research indicates that OSAHS modulates the levels of serum PCSK9. Individuals with OSAHS exhibit increased levels of serum PCSK9, which are positively associated with the extent of OSAHS. Serum PCSK9 levels might function as a straightforward and dependable biomarker for the onset, progression, and severity of OSAHS. Detecting PCSK9 levels in serum early could offer a novel and trustworthy foundation for the preventative, diagnostic, and therapeutic strategies against OSAHS.