
Regular physical activity is a well-known protective factor in the context of many cardiovascular diseases. Additionally, it has been proven to significantly reduce the risk of osteoporosis, type 2 diabetes, and cancers of the colon and breast. Premature all-cause mortality is reduced by 31% due to physical activity [1]. Studies have shown that it actively reduces symptoms associated with depression and anxiety disorders, leading to positive effects on mental health. [2]. However, according to the World Health Organization (WHO), more than a quarter of the global population does not engage in physical activity as recommended [3]. High levels of physical inactivity are also observed in the pediatric population [4]. The inactivity rates are highest in high-income regions, influenced by sedentary lifestyles and motorized transport, while low-income regions show more physical activity due to occupational and transportation needs. The global level of physically inactive individuals remained stable from 2001 to 2016, and for this reason, the authors recommend legislative actions aimed at promoting physical activity [5]. If the efforts of organizations such as the WHO are successful, the percentage of physically active individuals is likely to increase. Although the benefits of an active lifestyle are well known, it is also important to consider the potential risks.
The dangers related to sports concern both professional athletes and amateur athletes. However, distinguishing between amateur and professional athletes is challenging. Additionally, the concept of “shamateurism” has been introduced to describe amateur athletes who receive financial support from sponsors. Furthermore, state-sponsored programs in Eastern Bloc countries blurred these distinctions further. Athletes were formally amateurs employed in the military, for example, but were actually training full-time [6]. In some disciplines, it is strictly defined who the specific competitions are dedicated to, and athletes belonging to a given association are prohibited from participating in amateur competitions [7]. Additionally, there is a group of student-athletes who represent universities and are organized by the International University Sports Federation (FISU).
Physical activity, particularly sports competition, can increase the risk of various injuries within a given discipline. In the most tragic cases, it can even lead to the death of an athlete. The cause may be obvious, such as an injury, but death can also occur in an apparently healthy athlete without external factors, in which case sudden death should be suspected. Proper definition is very important to avoid errors in diagnosing the cause of death, and correctly classifying the cause of death facilitates retrospective research (Figure 1). The term “sudden” indicates that death occurs no later than 1 or 24 hours after the onset of symptoms. In the available literature, authors more often adopt the 1-hour limit, but definitions encompassing a 24-hour period also appear. It is a matter of debate whether the definition should include the term “witnessed”, as sudden death could only be confirmed in the presence of witnesses, which would exclude many deaths. Some authors also allow the 24-hour period only in the case of unwitnessed deaths. An exception to this time limit is the situation when sudden cardiac arrest (SCA) occurs, and sinus rhythm is restored through successful resuscitation, but the patient ultimately dies due to complications such as brain damage. Even though death occurred later than an hour after the onset of symptoms, it should be classified as sudden death, more precisely as aborted sudden death [8,9].
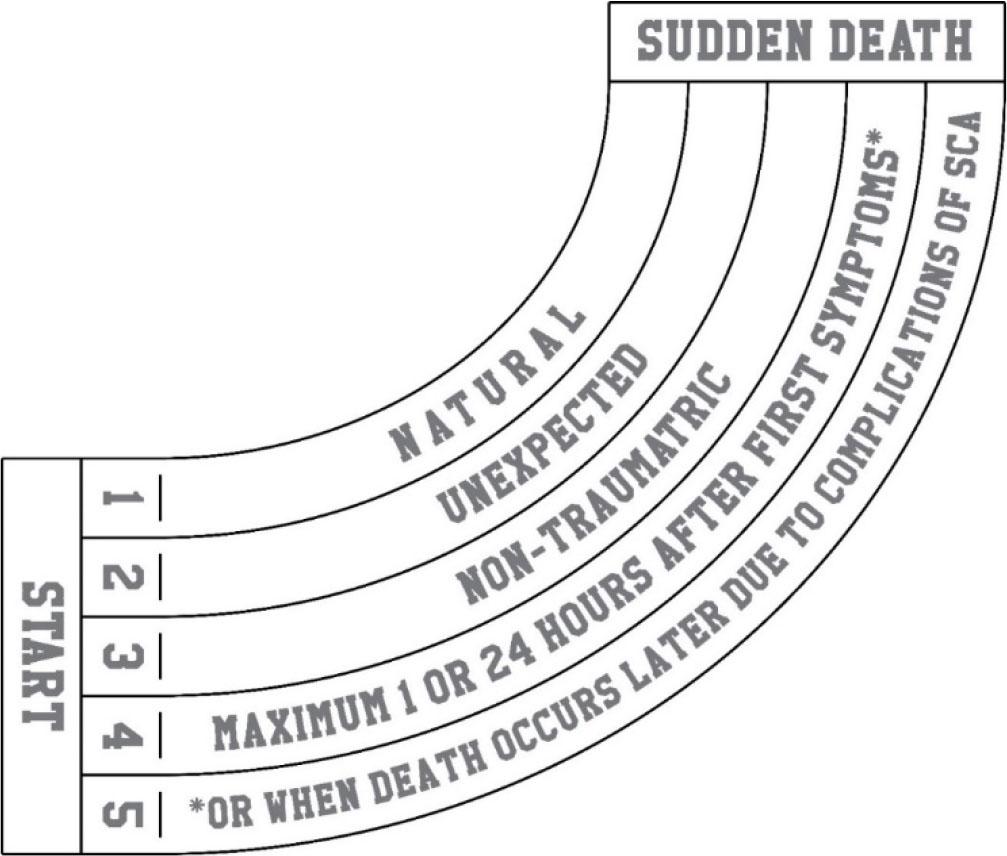
Key elements of the definition of sudden death
A narrower definition is sudden cardiac death, which indicates a cardiac or cardiovascular cause and is the most common cause of death within 1 hour of the onset of symptoms. All pathomechanisms lead to SCA, but the initial cause may come from another system in the body. For this reason, apart from sudden cardiac death, causes such as cerebral or respiratory should be considered.
The literature questions whether to classify patients with known diseases—where annual mortality is predictable in their group—as sudden deaths, even if they died soon after symptoms appeared. For this reason, some authors suggest that the definition should include the term “unexpected” [10]. This does not exclude all chronically ill patients, as the deaths of patients for whom such a quick death is not expected due to a given disease will be classified as sudden death.
The aim of the review was to assess the phenomenon of sudden death in sports with particular emphasis on epidemiology, typical etiologies, prevention methods, and postmortem diagnostic methods especially from a forensic perspective.
A literature review was conducted, which included searching databases such as PubMed, Medline, Scopus, and Google Scholar. The search was performed using Boolean operators using the following keywords: “sport”, “athlete”, “physical activity”, “exercise” “sudden death”, “sport-related death”, “cardiac”, “non-cardiac”, “pathology”, and “post-mortem diagnostics”. All types of peer-reviewed articles were allowed in the study, including case reports, original research, reviews, and guidelines published in journals with coverage in analyzed databases. Inclusion and exclusion criteria were established to identify the most relevant scientific articles and reviews, focusing on publications from the last 10 years. Moreover, the decision to include the work in the review was also based on the analysis of the degree of relevance with the topic of the study, level of evidence, size of the study group, research methodology used, scientific quality, elements of novelty, and clinical currentness. Particular attention was given to studies concerning the pathophysiology of sudden death in sports, prevention methods, and postmortem procedures. Studies that defined sudden death differently from the definition provided in the introduction were excluded from the selected literature. The review included papers that adopted the criterion of death within 1 hour or 24 hours from the onset of the first symptoms. Based on the overall analysis, a set of research works included in the study was selected as the most important for describing the issue.
Evaluating sudden death from an epidemiological perspective is challenging due to discrepancies in definitions, the lack of comprehensive medical information about patients, and an insufficient level of expanded diagnostics, such as autopsies or toxicological examinations. Sudden death is estimated to cause about 4–5 million deaths annually worldwide [11] and accounts for 20% of all deaths [12].
The incidence of sudden death is higher among men than among women, and the risk increases with age, except for a peak observed in the age group below 5 years, where the increase in fatal cases is due to sudden infant death syndrome (SIDS). Additionally, risk factors include a history of cardiovascular diseases, smoking, obesity, hypertension, and high cholesterol levels [11]. Of course, most of these risk factors are rare among professional athletes, but they can occur in individuals who engage in amateur sports.
Sports-related sudden death causes about 5% of all sudden deaths. Cases among recreational athletes significantly dominate (over 90%) compared to young, professional athletes (about 6%). This phenomenon occurs more frequently in male than in female athletes [13]. Different sports lead to sudden death in different countries, depending on the popularity of each sport in a given region. Based on studies conducted in Japan, the dominant sport where sudden death occurs among young athletes is basketball [14]. It also predominates in the United States of America (USA), with baseball being the second most common sport in this regard [15]. In contrast, in Spain, the highest number of fatal cases has been recorded among those practicing cycling, football, and jogging [16].
The most common causes of cardiac sports-related deaths vary according to age groups and the intensity of sports activity [17,18,19,20,21]. Studies suggest that coronary artery disease (CAD) is the most common cause of sports-related sudden cardiac death [19]. An analysis in Switzerland confirms this thesis, focusing on a population aged 10 to 50 years [22]. Similar conclusions are drawn from a study in Australia, where CAD accounts for 50% of sports-related sudden deaths among adults [17]. Another Swiss study additionally found that CAD was the most common cause of death in the 10–39 age group, both among recreational and competitive athletes [23]. Deaths among young individuals (defined as those under 35 years of age) occur mainly due to genetic risk factors and myocardial diseases, while in the older population, acquired pathological changes, particularly in the coronary arteries, dominate [18]. A study conducted in France showed that in the population under 30 years of age, the main cause of death during physical activity was cardiomyopathies, while in the older population, nearly half of the deaths were related to CAD [24]. Similar observations were made in a study conducted on a Chinese population, where cardiomyopathies dominated in the under-35 age group, and CAD was more prevalent among the older group [25]. A study from Spain also confirms this observation. In the population over 35 years of age, CAD accounted for nearly 85% of sports-related sudden deaths, compared to 13.5% in the under-35 age group [26].
In CAD, acute myocardial ischemia most often occurs due to the rupture of an atherosclerotic plaque, which constitutes embolic material in a major coronary artery. This is associated with the risk of developing polymorphic ventricular tachycardia. In such patients, particularly intense sports activity is an additional risk factor for sudden death. Post-exercise stunning is observed, leading to transient left ventricular contractility disorders. Intensive physical exertion in occasional athletes also leads to the activation of the coagulation system [27,28]. Such pathomechanisms typically occur during intense physical exertion. In contrast, moderate physical activity helps prevent CAD and is recommended as therapy for those diagnosed with it [29].
Apart from atherosclerosis-related etiologies, death can occur due to coronary artery vasculitis, anomalous coronary arteries, coronary artery dissection, or coronary artery spasm [30]. Vascular spasm is triggered by catecholamines such as adrenaline, released as a result of intense physical exertion and stress. This phenomenon is difficult to diagnose in primary prevention studies in athletes and undetectable postmortem [31]. Vessel lumen narrowing can also occur due to anatomical anomalies such as myocardial bridges. Additionally, the compression caused by myocardial bridges leads to turbulent blood flow, which promotes the development of atherosclerotic changes in the vessel proximal to the site of compression [32].
Intense physical exertion significantly increases the body’s oxygen demand, including that of the heart muscle. During sports activities, coronary blood flow increases fivefold. In a healthy person, this relationship does not lead to complications. However, in the case of a narrowed blood vessel, the required amount of oxygen cannot be delivered during exertion. In such a situation, resting electrocardiogram (ECG) does not show signs of myocardial ischemia, and ECG changes begin to appear during a stress test [33].
There are, however, studies indicating that cardiomyopathies overall constitute the most common cardiovascular cause of sports-related sudden deaths [34,35], with hypertrophic cardiomyopathy being the most common cause of sudden death among young athletes [36]. Hypertrophic cardiomyopathy is characterized by pathological thickening of the heart walls, which can lead to left ventricular outflow obstruction and conduction disorders, particularly in the area of the His bundle. In this disease, death most often occurs due to conduction disturbances leading to ventricular fibrillation. Among fatal cases of hypertrophic cardiomyopathy, only 20% had this condition diagnosed during life, and in one out of four patients, symptoms such as palpitations, syncope, dyspnea, and chest pain were previously present. Most deaths were observed at rest, while during sports activities, sudden death occurred most frequently among young athletes aged 10–15 [37]. Among cardiomyopathies, the second most common cause of death is arrhythmogenic cardiomyopathy, in which myocytes are replaced by fibrofatty tissue. The abnormal tissue can lead to macro-reentrant circuits, resulting in sustained ventricular tachycardia [38]. Half of the patients with arrhythmogenic cardiomyopathy are diagnosed postmortem, with symptoms occurring in only one in four patients during life. Although the main circumstance of death is not physical activity but performing daily activities, athletes have a 5.4 times higher risk of death from this etiology than non-active individuals [39]. A much rarer cause of sudden death is dilated cardiomyopathy, characterized by the enlargement of the left ventricle with systolic dysfunction. The most common heart rhythm disorder is ventricular tachycardia, which occurs via a reentry mechanism due to hypertrophy and replacement fibrosis [40].
Deaths due to myocarditis mainly affect young and physically active individuals. Myocarditis can occur, among other reasons, as a complication of infectious diseases or drug injections. Owing to the lack of specific symptoms, clinical diagnosis of this condition can be problematic. It is crucial to avoid physical exertion during the recovery period [41,42]. There have also been cases of sudden death due to infiltrative heart diseases such as sarcoidosis and amyloidosis. In sarcoidosis, the lungs and lymphatic system are mainly affected, and heart involvement is less common, with isolated cardiac involvement being extremely rare. Heart involvement can lead to myocarditis with conduction disorders. Changes similar to dilated cardiomyopathy and arrhythmogenic right ventricular cardiomyopathy are also observed. Sarcoidosis can also lead to coronary artery dissection [43]. The risk of sudden death in sarcoidosis patients, depending on the sources, is the same as in the general population or slightly increased [44,45].
In long-QT syndrome, the heart’s action potential is prolonged, observable in an ECG. This prolongation leads to delayed repolarization, causing early afterdepolarizations. This results in rhythm disturbances, mainly torsades de pointes. The heart usually returns to a normal rhythm after such an episode, but torsades de pointes can develop into ventricular fibrillation. Increased mortality is observed among long-QT syndrome patients aged 20 years, with no history of syncope and a QTc of less than 500 ms [46]. In short-QT syndrome, the ECG shows a shortened QT interval. The shortening of the heart’s action potential leads to disorganized cardiac muscle activity, significantly reducing its efficiency. This is associated with a risk of ventricular or atrial fibrillation. The most common and often the only symptom of this condition is cardiac arrest, leading to sudden death. Syncope occurs in less than 25% of patients [47]. In Brugada syndrome, death most commonly occurs due to the onset of polymorphic ventricular tachycardia or ventricular fibrillation. It accounts for 4% of all sudden deaths. A history of cardiogenic syncope may be a risk factor. Proper diagnosis of syncope is essential since vasovagal syncope does not increase the risk of sudden death. However, syncope is present in the history of only one-third of patients [48,49].
Undiagnosed aortic aneurysms increase the risk of sudden death in athletes. In disciplines where aerobic effort predominates, a rise in blood pressure is observed. However, it does not reach the same level as during strength training. At the site of vessel dilation, the vessel walls weaken and elevated blood pressure increases the risk of rupture, leading to aortic dissection. Studies have confirmed that physical exertion and stress are risk factors for sudden death via this mechanism [50].
Sudden death is always associated with cardiac arrest. However, its underlying cause does not necessarily have to be cardiological. For this reason, cases of sudden death are also attributed to neurological, metabolic, endocrine, respiratory, and immunological causes [51].
Non-cardiac etiologies of death are most commonly recorded due to epilepsy and are termed sudden unexpected death in epilepsy (SUDEP) [51]. Nonetheless, physical activity has a positive impact on the course of the disease. Studies show that people who engage in sports experience fewer seizures. However, it is important to consider epilepsy as a cause of death and to conduct proper differential diagnosis, as syncope, such as cardiogenic syncope, may be mistakenly diagnosed as a seizure. While regular physical activity improves the course of the disease, it does not exclude the occurrence of SUDEP during sports. The underlying cause is neurological—a dysregulation of the nervous system, resulting in arrhythmias such as paroxysmal asystole and impaired breathing. Vagal nerve stimulation leading to bradycardia and, in the most dramatic cases, cardiac arrest is also observed [52,53,54].
A type of hemorrhagic stroke, intracerebral hemorrhage occurs with similar frequency. This is the most common type of stroke in children and young adults [55]. In cases of brain edema, loss of autonomous central respiratory function occurs, followed by a slowing of heart rate leading to asystole. Studies show that physical activity is a protective factor against stroke [56]. In static disciplines like weightlifting, a sudden increase in blood pressure occurs. This mechanism raises the risk of strokes, including intracerebral and subarachnoid hemorrhages [57]. Contact sports increase the risk of ischemic stroke, such as American football or boxing. A stroke leading to death through sudden death mechanisms is difficult to link to injuries sustained during sports, as it occurs after a significant time interval from these injuries [58].
Some authors also highlight that dehydration and electrolyte imbalances can result in death in worst-case scenarios. Cases have been reported in marathon runners who suffered ischemic strokes with no other identified cause than dehydration induced by extreme physical exertion [59]. Prolonged physical exertion, especially in warm climates, and the use of hypotonic fluids can lead to exercise-associated hyponatremia (EAH), which is associated with the risk of brain edema [60].
Sudden death through respiratory mechanisms is relatively rare. It mainly occurs due to pulmonary embolism or asthma. Athletes are at higher risk for exercise-induced asthma (EIA) and exercise-induced bronchospasm (EIB) [61]. Fatal cases due to asthma have been recorded in athletes, but they are very rare. It is generally accepted that physical activity is safe for asthma patients and can improve the course of the disease [62].
According to the definition of anaphylaxis, symptoms involve multiple systems; thus, the underlying cause is immunological (with a non-immunological form also recognized), leading to dysfunctions in systems such as respiratory, gastrointestinal, or cardiovascular, which can result in sudden death. Individuals engaging in physical activity are at risk for exercise-induced anaphylaxis, where anaphylaxis is triggered by physical exertion. A subcategory of this phenomenon is food-dependent exercise-induced anaphylaxis (FDEIA), where anaphylaxis occurs when an allergenic food is consumed before physical activity [63]. Additionally, participating in outdoor sports involves exposure to various airborne allergens and venoms [64].
Another non-cardiac cause is rhabdomyolysis, where significant amounts of myoglobin are released into the blood due to muscle damage, leading to acute kidney failure [65,66,67]. Sickle cell anemia should also be considered a predisposing factor for sudden death during physical activity [68].
Doping in sports, which involves the use of prohibited substances and methods to enhance physical performance, represents a serious problem not only ethically but also health-wise. This phenomenon is observed among both professional athletes and amateur athletes [69]. Combating unfair practices poses a significant challenge as new doping methods are developed to circumvent increasingly stringent bans. This subsection will describe only selected forms of doping that can lead to sudden death.
Sudden death caused by the abuse of erythropoietin (EPO) is a significant threat to athletes specializing in endurance aerobic sports. Erythropoietin is a hormone naturally occurring in the body that stimulates the production of red blood cells, thereby improving the blood’s oxygen transport capacity. However, using synthetic EPO as a doping agent leads to a pathological increase in the number of red blood cells, which translates into increased blood viscosity. Such changes in the rheological parameters of blood are associated with the risk of hypertension, heart failure, myocardial infarction, and thromboembolic events. Dehydration during training or competition can predispose one to sudden death [70].
In individuals using anabolic androgenic steroids (AAS), elevated D-dimers are observed, suggesting an increased risk of venous thromboembolism. However, because of the observed changes in both procoagulant and anticoagulant factors, there are doubts in this regard [71]. Death can occur due to the narrowing of coronary vessels through various mechanisms. The first mechanism is coronary artery spasm, to which individuals using AAS are more predisposed. An increased risk of atherosclerotic plaque formation has also been observed, which can serve as embolic material [72,73].
Salbutamol is not completely banned, but specific doses are allowed for athletes, and a maximum concentration in urine has been set for anti-doping control. Using this selective and short-acting agonist of β2-adrenergic receptors (SABA) in higher doses leads to tachycardia with QT interval prolongation and angina pectoris, while metabolic disturbances such as hypokalemia can be dangerous. Acute overdose causes sinus tachycardia, myocardial ischemia, and ventricular and supraventricular tachycardia, which potentially can lead to sudden death [61].
Abuse of substances not included on the World Anti-Doping Agency (WADA) prohibited list can also have serious health consequences. For example, one of the most popular stimulants globally, caffeine, is present in many preparations dedicated to athletes, such as caffeine shots or energy gels. Additionally, companies producing energy drinks base their marketing on sponsoring athletes in various disciplines. The effects on the cardiovascular system include decreased or increased heart rate, increased blood pressure, and changes in the morphology of the ECG ST-T segment. These factors increase the risk of sudden cardiac death, and overdosing on this substance has led to recorded fatal cases [74].
Each case of sudden death among athletes is not only a personal tragedy but also a clear alarm signal for the entire sports community, indicating the need for increased efforts in preventive measures, both primary and secondary. The regulations for sports participation qualification are strictly regulated by law and vary depending on the country. However, the primary issue is the lack of mandatory medical examinations for participation in some amateur-level competitions. For example, in marathons organized in the five largest cities in Poland, none of the regulations require participants to undergo any medical examinations. In this country, professional sports require medical examinations. An initial examination is conducted and then repeated every 24 months (every 6 months if required by the health condition or the specifics of the sports competition). It is crucial to gather a detailed medical history, with an emphasis on the occurrence and characteristics of fainting, loss of consciousness, heart palpitations, dizziness, and shortness of breath. However, many of the previously described medical conditions are asymptomatic, and the first symptom may be sudden death. In addition to the basic medical examination, supplementary tests such as a 12-lead ECG, complete blood count with differential, serum glucose concentration, and urinalysis are performed. For divers, spirometry is conducted, and in combat sports, a neurological examination is performed [75,76]. Some of the previously described cardiac causes potentially leading to sudden death can be detected through ECG examination. Increasing the sensitivity of heart disease screening would involve extending the examination to include echocardiography [77].
Most victims of sudden death did not have a diagnosed heart disease, making it particularly difficult to estimate the risk of death in this group [78]. In heart diseases where the risk of sudden death is assessed as high, there are indications for the implantation of an implantable cardioverter-defibrillator (ICD). This can serve as both primary prevention, e.g., in patients with cardiomyopathy or channelopathies, and secondary prevention in patients with a history of SCA [79,80]. Wearable cardioverter-defibrillators are also available on the market and are used in patients who do not qualify for an ICD [81,82]. For patients diagnosed with aortic dilation, it is recommended for them to lift weights not exceeding 50% of their body weight to prevent aortic dissection [50]. Patients with a history of anaphylaxis should always carry adrenaline, preferably in the form of auto-injectors [83], and asthmatic patients should always have medications for interrupting a potential asthma attack—such as inhaled corticosteroids (ICS) and short-acting beta-agonists (SABA)—and if they experience exercise-induced bronchoconstriction (EIB), they should use SABA before exercise [84]. Many factors cause sudden death, and it is not possible to conduct a screening among athletes that would ensure sudden death does not occur during physical activity. For this reason, members of the sports community should be able to perform basic life support (BLS) and that sports facilities be equipped with automated external defibrillators (AEDs) [85,86].
Postmortem diagnosis of sudden death cases in sports can pose significant diagnostic challenges due to the broad differential diagnosis and the frequent absence of characteristic symptoms [87]. To appropriately direct postmortem diagnostics, it becomes crucial to analyze the circumstances surrounding the death and the deceased’s medical history. Information regarding the course of the event and the circumstances of death can come from witnesses or individuals providing first aid on the scene. Additionally, a detailed analysis of medical records regarding chronic diseases, previous procedures, or medications used by the deceased will help identify risk factors and guide further diagnostics [26,88,89]. Consideration should also be given to situations where sudden death during physical activity was the only episode of an undiagnosed disease [24,41]. Cardiological causes relate to abnormal heart function due to, for example, insufficient oxygen supply or functional rhythm disorders of various origins [87,90]. In such cases, examining the heart becomes a crucial step in the autopsy [89]. One of the first steps involves taking precise measurements of the organ’s dimensions, mass, and ventricular wall thickness to identify signs of heart hypertrophy and cardiomyopathy [91,92]. Next, the heart is dissected to assess the contents of the heart chambers and valves. A thorough evaluation of the coronary vessels is also essential, focusing on identifying anatomical anomalies and markers of atherosclerosis significantly narrowing the vessel lumen. Non-atherosclerotic coronary lesions related to diseases such as Kawasaki disease or the presence of myocardial bridges should also be assessed [24]. A study conducted in Australia showed that approximately 25% of sports-related sudden death cases involved a heart mass exceeding 500 g [17]. Additionally, distinguishing between cardiomyopathy and Athlete’s heart, resulting from physiological adaptive changes due to regular physical exertion, is crucial in heart evaluation [93,94]. Histopathological examination samples should be taken to assess the presence of fibrosis markers, inflammation, or fresh ischemic foci. In the case of deaths during physical activity in children and young adults, it is also important to search for congenital heart defects and coronary vessel anomalies [22,95,96]. Moreover, if the heart examination remains inconclusive without visible macroscopic changes in the heart, the possibility of molecular causes underlying diseases such as Brugada syndrome or long-QT syndrome should be considered [18,93,97]. In such cases, detailed genetic testing can be performed as part of a molecular autopsy to determine the presence of structural and arrhythmogenic diseases, including channelopathies [88]. If the individual involved in sports had an implanted cardiac electronic device, a postmortem reading of its record can provide important information about heart function just before death [98]. Collecting material (e.g., blood, urine, and vitreous humor) for toxicological testing to identify drugs or other performance-enhancing substances also becomes a crucial element in postmortem diagnostics [88,99].
Furthermore, specific situations arise depending on the sport discipline. In water sports such as swimming, death can result from an acute condition, exacerbation of an underlying disease, or drowning [95,100]. Potential cause of drowning includes an accident or loss of consciousness due to a medical condition. In such cases, lung examination becomes crucial to search for typical signs of drowning and other features of water aspiration into the respiratory system.
In sports like diving, in addition to the possibility of an acute medical condition, death can result from equipment failure or improper diver behavior leading to barotrauma, decompression sickness, and gas embolism. In such cases, the autopsy may be inconclusive, and assessing its results in relation to the diving equipment analysis and computer record becomes crucial [101,102,103,104].
Other important cases include contact sports and martial arts (e.g., boxing), where death can result from injuries. In such cases, the injuries should be visible and assessed along with their severity during the autopsy [95]. Death caused directly by trauma does not fall under the definition of sudden death, which refers to non-traumatic causes. However, considering other causes is also important.
In high-altitude sports, death can also result from hypothermia or acute mountain sickness with brain or lung edema [105,106]. Additionally, during climbing, accidents and falls from heights can cause severe injuries. Determining the cause of the fall and whether it was due to an undiagnosed disease is important [107].
Another category includes endurance sports, where prolonged exertion can lead to dehydration with subsequent electrolyte imbalance, for which there are no specific changes detected during autopsy [95].
This review has several limitations that need to be considered when interpreting the findings. First, the included studies vary significantly in terms of design, population, and diagnostic criteria for sudden death in sports, which may introduce heterogeneity and impact the comparability of results. Second, the reliance on retrospective data in some studies may lead to incomplete or inaccurate reporting of cases and causes of sudden death. Moreover, the quality of the postmortem examinations varied across studies, potentially affecting the accuracy of the identified causes of death. Additionally, variations in the methodologies used to assess and classify the causes of sudden death may have led to inconsistencies in the findings. The relatively small sample sizes of some studies also limit the generalizability of the results. Furthermore, the lack of detailed individual-level data in many studies prevents a more nuanced analysis of risk factors and their interactions. Another limitation is the potential for confounding variables that were not controlled for in the original studies, such as the level of training, underlying health conditions, and environmental factors. Lastly, the language and publication date restrictions imposed during the literature search might have led to the exclusion of relevant studies, particularly those published in languages other than English or outside the selected time frame. Future research should aim to address these limitations by standardizing definitions and diagnostic criteria, improving the quality and consistency of data collection, and including a broader range of studies to ensure a more comprehensive understanding of the issue.
Both in the general population and among athletes, the predominant cause of sudden death is of cardiac origin. The risks associated with sports are not limited to elite competition but also affect amateur athletes. This knowledge should prompt more detailed screening, which could significantly contribute to preventing such tragic events. However, there is a lack of standardized definition of sudden death in sports, which hinders precise data collection and comparison of research results. Standardizing definitions and diagnostic criteria is essential to improve the quality of epidemiological studies and enable more effective preventive actions. It is necessary to maintain registries that provide accurate information on the frequency and causes of sudden deaths among athletes. It is recommended that athletes, coaches, sports organizations, and medical personnel focus on several key areas. Primarily, expanding systematic screening to identify athletes at potential risk of sudden death is crucial. It is also important to regularly conduct first aid training, especially in the use of AEDs, which should be readily available during sporting events. Increasing awareness of the risks associated with doping is also essential, as the use of substances such as EPO and anabolic steroids can lead to life-threatening complications.