
Thailand is undergoing a rapid demographic transition toward an aging society. As of 2023, nearly 19.97% of the population was aged 60 years and older, indicating that the country is approaching a super-aged society.1 This demographic shift presents significant challenges for health and social systems, particularly regarding non-communicable diseases (NCDs), which are prevalent among older adults.2,3 In addition to these physical health concerns, it is crucial to maintain robust social networks to ensure successful aging and overall well-being.4,5
Social isolation—defined as an objective lack of social relationships or infrequent social interactions—has been strongly linked to increased risks of mortality, functional decline, and poor mental health in older populations.6 Although distinct from loneliness, which reflects a subjective sense of social disconnection, the two phenomena are often interrelated.7 Both are recognized as major public health concerns due to their detrimental effects on health outcomes and quality of life in later life.8 Older adults with NCDs are especially vulnerable to social isolation due to limited mobility, chronic disease burden, and frequent interactions with the healthcare system, all of which can restrict their participation in social activities.
Accurate identification of socially isolated individuals requires brief, reliable, and culturally appropriate assessment tools. The Lubben Social Network Scale (LSNS) is one of the most widely used instruments for this purpose. Its abbreviated version, the LSNS-6, includes 6 items assessing the size and closeness of an individual’s social network, divided into two subscales: family and friends.9 Each subscale comprises 3 items measuring perceived availability of social contact and support. Validation studies conducted in China,10 Mongolia,11 and Puerto Rico12 have demonstrated the LSNS-6’s strong psychometric properties, supporting its cross-cultural applicability.
Despite its broad international use, the LSNS-6 has not yet been psychometrically validated for use in the Thai context, particularly among older adults living with NCDs. Given the cultural differences in family structure and social norms in Thailand, it is essential to determine whether the LSNS-6 maintains validity and reliability in this population. In the context of home health care, assessing social connectedness is especially important, as socially isolated individuals are at greater risk of poor treatment adherence, hospital readmissions, and diminished quality of life. The LSNS-6 offers a brief, evidencebased screening tool that can be integrated into home visits or telehealth assessments to identify at-risk individuals and guide timely intervention strategies.
Therefore, the present study aimed to evaluate the construct validity, internal consistency, and composite reliability (ρc) of the Thai version of the LSNS-6 among community-dwelling older adults with NCDs. It was hypothesized that a two-factor model—comprising family and friend subscales—would exhibit good model fit and demonstrate satisfactory reliability indices.
This psychometric validation utilized a cross-sectional design, drawing on data from a previous study involving older adults with NCDs in Thailand.13 A total of 250 community-dwelling adults aged 60 years and older were recruited using multistage stratified sampling from both urban and rural communities in Ubon Ratchathani Province. Inclusion criteria were: (a) a confirmed diagnosis of at least one NCD (e.g. hypertension, diabetes mellitus), (b) the ability to communicate in Thai, and (c) sufficient cognitive function to participate in an interview. Individuals with severe sensory impairments or significant cognitive decline were excluded.
The Lubben Social Network Scale-6 (LSNS-6) is a brief instrument designed to assess the size and closeness of an individual’s social network. It comprises 6 items divided into two subscales: Family (3 items) and Friends (3 items). Each item evaluates the number of people in the respondent’s network who (a) interact regularly, (b) can be called on for help, and (c) provide personal support. Responses are rated on a 6-point scale (0 = none to 5 = nine or more), yielding a total score ranging from 0 to 30. Scores below 12 indicate a high risk of social isolation.9
Demographic variables were also collected to describe the sample and examine population diversity. These included age, sex, marital status, educational attainment, monthly household income, and residential setting (urban or rural).
The LSNS-6 was translated into Thai using established cross-cultural adaptation guidelines.14 Two bilingual experts independently translated the instrument from English to Thai, followed by synthesis into a single version after resolving discrepancies. A third bilingual translator, blinded to the original version, performed a back-translation to English. An expert panel of 8 specialists in aging, gerontology, and psychometrics reviewed the translated version for content validity, cultural appropriateness, and clarity. Content Validity Indices were calculated: item-level CVI (I-CVI) ranged from 0.88 to 1.00, and the scale-level CVI (S-CVI/Ave) was 0.95, indicating excellent expert agreement. Minor adjustments were made to improve clarity. The prefinal Thai version was then pilot-tested with 30 older adults, confirming comprehensibility and interpretability.
Trained interviewers administered structured, face-to-face questionnaires in participants’ homes or community centers. Data collection included demographic information and LSNS-6 responses, all completed in a single session.
Data analyzes were conducted using IBM SPSS Statistics version 26 for descriptive and reliability analyzes, and AMOS version 24 for confirmatory factor analysis (CFA). Descriptive statistics summarized demographics and LSNS-6 item characteristics. The distribution of each item was assessed for normality based on skewness and kurtosis values within the range of ±2. The construct validity of the LSNS-6 was evaluated through CFA, which tested the proposed two-factor model consisting of family and friend subscales. Model fit was assessed using several goodness-of-fit indices: chisquare to degrees of freedom ratio (χ2/df), root mean square error of approximation (RMSEA), standardized root mean square residual (SRMR), comparative fit index (CFI), and Tucker–Lewis index (TLI). Acceptable model fit thresholds were based on Hu and Bentler15 and Kline16, included χ2/df values less than 3, RMSEA and SRMR values of 0.08 or below, and CFI and TLI values of 0.95 or higher. Internal consistency reliability was measured using Cronbach’s alpha, with values of 0.70 or greater deemed acceptable. Additionally, ρc and average variance extracted (AVE) were calculated for the family and friend subscales to evaluate convergent validity, with recommended minimum values set at 0.70 for ρc and 0.50 for AVE. Missing data were minimal (<5%) and addressed using listwise deletion in both CFA and reliability analyzes. Statistical significance was set at P < 0.05.
The study included 250 community-dwelling older adults with diagnosed NCDs, with a mean age of 69.61 years (SD = 7.47). The majority of participants were female (63.6%) and married (55.2%), followed by widowed (27.6%) and single/divorced (17.2%). Educational attainment was primarily at the primary level (66.4%), with 23.2% having completed secondary education and 10.4% holding higher education degrees. Regarding monthly household income, 82.8% earned less than 5000 THB, 8.0% earned between 5001 and 10,000 THB, and 9.2% earned over 10,000 THB. Participants were equally distributed between rural and urban communities (50.0% each).
All six LSNS-6 items demonstrated adequate distributional properties, with skewness and kurtosis values within the acceptable range (±2). Items ranged from 2.6 to 4.1 on a scale from 0 to 5. Corrected item-total correlations ranged from 0.58 to 0.73, exceeding the recommended threshold of 0.30, indicating good homogeneity among items.
The hypothesized two-factor structure demonstrated excellent fit: χ2/df = 1.82, RMSEA=0.045, SRMR = 0.038, CFI = 0.981, TLI = 0.970, GFI = 0.953 (Figure 1). All standardized factor loadings were statistically significant (P < 0.001) and exceeded 0.70, with loadings ranging from 0.80 to 0.84. The squared multiple correlations (R2) indicated that their respective factors explained between 64% and 70% of the variance in each item (Table 1).
Standardized factor loadings and R2 for LSNS-6 items (two-factor model).
| Item | Factor loading (λ) | R2 |
|---|---|---|
| Family subscale | ||
| 1. How many relatives do you see/hear from monthly? | 0.80* | 0.64 |
| 2. How many relatives do you feel close to? | 0.82* | 0.67 |
| 3. How many relatives could you call for help? | 0.83* | 0.69 |
| Friends subscale | ||
| 4. How many friends do you see/hear from monthly? | 0.81* | 0.66 |
| 5. How many friends do you feel close to? | 0.84* | 0.70 |
| 6. How many friends could you call for help? | 0.83* | 0.69 |
Note: LSNS-6, Lubben Social Network Scale-6;
indicates standardized factor loadings significant at P < 0.001.
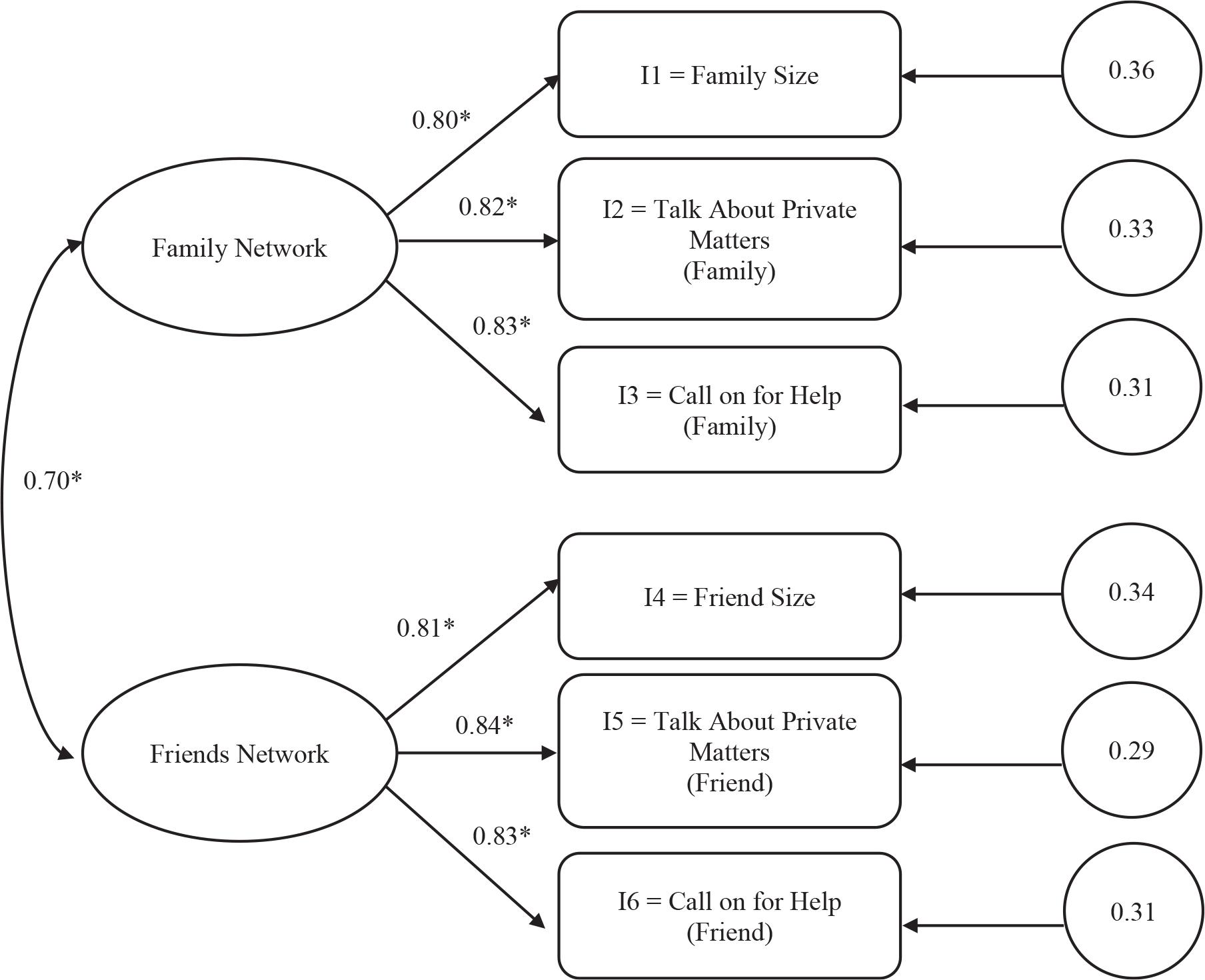
CFA of LSNS-6 Two-Factor Model (family and friends).
Note: Standardized loadings and error variances are shown. P < 0.001. CFA, Confirmatory factor analysis; LSNS-6, Lubben Social Network Scale-6.
The Thai LSNS-6 demonstrated strong internal consistency, with Cronbach’s alpha = 0.88 for the total scale, 0.85 for the Family subscale, and 0.88 for the Friends subscale. ρc for the overall model was 0.85, and the AVE was 0.67, surpassing recommended thresholds (Table 2). These results confirm that the Thai LSNS-6 possesses adequate internal consistency and convergent validity.
Reliability indices for LSNS-6 and subscales.
| Scale | Cronbach’s α | ρc | AVE |
|---|---|---|---|
| LSNS-6 total | 0.88 | 0.85 | 0.67 |
| Family subscale | 0.85 | 0.84 | 0.65 |
| Friends subscale | 0.88 | 0.86 | 0.68 |
Note: AVE, average variance extracted; LSNS-6, Lubben Social Network Scale-6; ρc, composite reliability.
This study aimed to validate the Thai version of the LSNS-6 among community-dwelling older adults with NCDs. The findings demonstrate that the LSNS-6 has strong psychometric properties in this population, aligning with evidence from previous international validation studies.
The results of the CFA provided strong support for the proposed two-factor model, which delineates the family and friends domains as initially suggested Lubben et al.9 This framework is consistent with previous validations conducted across various cultural contexts, including studies in China,10 Mongolia,11 and Puerto Rico.12 It suggests that the conceptualization of social networks as two interconnected yet distinct dimensions holds universal applicability. Model fit indices revealed an excellent fit to the data. The RMSEA (0.045) and SRMR (0.038) indicate close fit, while CFI (0.981) and TLI (0.970) exceed 0.95, demonstrating excellent model fit, exceeding the minimum criteria recommended for robust structural validity15 and affirming that the Thai-LSNS-6 effectively captures the theoretical foundation of social network constructs. Additionally, all standardized factor loadings were significant, ranging from 0.80 to 0.84, which surpasses the commonly accepted threshold of 0.70.17 This indicates that each item substantially contributes to its respective latent factor. Notably, the family related items exhibited slightly higher loadings compared to the friend-related items, likely reflecting the cultural importance of kinship ties in Thai society, where older adults traditionally depend on their families for emotional and instrumental support.18
The Thai-LSNS-6 exhibited excellent internal consistency, with Cronbach’s alpha values exceeding 0.85 for both the overall scale and its subscales. These values not only surpass the generally accepted threshold of 0.70 for research instruments19 but also indicate a strong homogeneity among the items. The reliability demonstrated in this study is comparable to or slightly higher than that observed in international validations, such as those conducted in China (α = 0.83)10 and Mongolia (α = 0.84),11 highlighting the stability of the LSNS-6 across different cultural contexts. In addition to Cronbach’s alpha, the ρc = 0.85 further affirmed the robustness of the measurement model, while the AVE = 0.67 surpassed the recommended cutoff of 0.50,17 thereby providing evidence of convergent validity. Collectively, these metrics indicate that the LSNS-6 items consistently reflect their underlying constructs (family and friends) and share a considerable proportion of variance with their latent factors.
The strong emphasis on family cohesion in Thailand is evident in the significant loadings for family related items, highlighting the pivotal role of kinship networks in the lives of older adults.18 In Thai society, family members—especially adult children—are traditionally seen as the primary providers of emotional, financial, and caregiving support.2,20 This cultural norm likely accounts for the continued prominence of familial ties within the social networks of older adults, even those managing chronic illnesses.13
Notably, the friend subscale also exhibited robust loadings and reliability, indicating that non-familial relationships play a crucial role in social connectedness. This observation aligns with global findings that suggest friendships offer unique benefits, such as companionship and emotional support, which complement familial bonds.21 For older adults in Thailand, the importance of nurturing and maintaining friendships may grow as urban migration and geographic mobility limit opportunities for daily family interactions.
The differentiation between family and friend networks carries significant implications for policy and practice. Interventions aimed at preventing social isolation among older Thais should not only strengthen family support systems but also foster opportunities for peer engagement—such as community clubs, volunteer initiatives, or neighborhood networks. Addressing both aspects provides a more comprehensive strategy for promoting healthy aging and alleviating isolation in a changing social landscape.
The validated Thai LSNS-6 provides a practical and culturally sensitive tool for home health care professionals to assess social isolation during home visits or remote consultations. Early detection of socially isolated older adults enables care teams to develop personalized care plans that integrate social support, caregiver involvement, and community resources. Incorporating this tool into home health care protocols can help reduce unnecessary hospital admissions and enhance overall health outcomes for patients with chronic conditions who are living at home. Furthermore, home care agencies can leverage LSNS-6 data for effective care coordination and outcome monitoring, ensuring that social well-being is recognized as a fundamental aspect of comprehensive home-based care.
This study boasts several strengths that bolster confidence in its findings. Firstly, the translation and cultural adaptation of the LSNS-6 adhered to rigorous, standardized procedures, including forward–backward translation, expert panel evaluation, and pilot testing with older adults with NCDs. This meticulous approach ensures both semantic and conceptual equivalence. Secondly, the application of CFA and multiple reliability indices is consistent with best practices in psychometric evaluation, thereby enhancing the validity of the conclusions drawn. Moreover, the inclusion of a relatively large sample of older adults with NCDs further amplifies the practical relevance of the findings for clinical and public health contexts in Thailand.
However, certain limitations should be acknowledged. First, the sample was drawn exclusively from Ubon Ratchathani Province in northeastern Thailand, which may limit the generalizability of the findings to other regions with different sociocultural, economic, and healthcare contexts. Future research should expand the sampling frame to include a broader and more diverse population across multiple provinces to enhance external validity. Second, the LSNS-6 items use ordinal response categories, which were treated as continuous data in the CFA. While this is a common approach in psychometric research, it may not fully capture the categorical nature of the data. Third, the cross-sectional design precludes assessment of test–retest reliability and predictive validity, limiting conclusions about the scale’s temporal stability and responsiveness to change. Longitudinal studies are recommended to evaluate these properties. Fourth, while face-to-face interviews were used to minimize misunderstanding, reliance on self-reported data may still introduce recall or social desirability bias. Fifth, although this study recognizes the importance of subgroup analyzes, it was unable to conduct additional robustness testing—such as measurement invariance across demographic characteristics, including income and education. Future research should evaluate the measurement invariance of the Thai LSNS-6 across key subgroups, including gender, age, and residential setting, to ensure consistent performance across diverse populations. Moreover, studies assessing the scale’s predictive validity are needed to determine whether LSNS-6 scores can reliably forecast relevant outcomes such as depression, hospitalization, or diminished quality of life. Finally, examining the practical integration of the LSNS-6 into clinical workflows and public health initiatives could support its broader use as a screening tool to inform targeted interventions and strategies for preventing social isolation among older adults.
The findings of this study provide strong support for the Thai LSNS-6 as a valid and reliable instrument for assessing social networks among community-dwelling older adults with NCDs. CFA affirmed a two-factor structure (family and friends) with excellent model fit, and internal consistency exceeded established psychometric benchmarks. Although the results are promising, further validation is needed—particularly test–retest reliability, predictive validity, and generalizability to broader populations. Beyond its research utility, the Thai LSNS-6 offers practical value for home health care providers, enabling the early identification of socially isolated individuals and informing tailored interventions to improve health outcomes. Future studies should explore its application in multidisciplinary care models and community-based screening initiatives.