
Ischemic stroke is a common condition leading to central nervous system damage, often accompanied by depressive symptoms. With the aging population, the mental health issues of stroke patients are receiving increasing attention, and depression has become one of the common complications following stroke.1 Traditional treatment methods primarily focus on pharmacological therapy, but recent studies have shown that environmental factors play a crucial role in neural recovery and the improvement of psychological states. Environmental enrichment, as an effective rehabilitation intervention, provides rich external stimuli that promote neuroplasticity and brain function recovery, demonstrating good efficacy in animal models.2–5
In animal experiments with ischemic stroke, environmental enrichment has been shown not only to improve cognitive function but also to significantly alleviate depressive behaviors. Studies have indicated that rats often exhibit typical depressive-like behaviors such as reduced sucrose consumption and decreased activity after ischemia-reperfusion, but environmental enrichment can significantly improve these behaviors. For instance, sucrose consumption tests show that environmental enrichment restores drinking preferences, while open field tests (OFTs) reveal restored activity levels close to normal. These changes reflect the positive impact of environmental enrichment on both neural and emotional functions.6–8
This study focuses on the effect of nursing intervention based on the concept of environmental enrichment on depressive behavior in rats with ischemic stroke. Using behavioral evaluation methods such as the sucrose consumption test and OFT, we further explore the efficacy of environmental enrichment intervention in alleviating depressive symptoms after stroke. The study’s results indicate that environmental enrichment intervention significantly improves rats’ emotional state and activity abilities, suggesting substantial clinical application potential. In the future, environmental enrichment-based intervention methods are expected to provide new therapeutic strategies for the management of depressive symptoms in ischemic stroke patients, especially in the management of neuropsychiatric symptoms.
This experiment has been reviewed and approved by the Animal Ethics Committee of Xuzhou Medical University, with ethical approval number [JSNU-IACUC-2024235]. All experimental procedures strictly adhere to animal ethics principles, minimizing the number of animals used, optimizing the experimental design to reduce animal suffering, and ensuring animal welfare. Male SD rats (2–3 months old) (provided by the Laboratory Animal Center of Xuzhou Medical University, Animal Use License No.: SYXK 2002–0038) were used. The fourvessel occlusion (4-VO) ischemia-reperfusion model9 was established as follows: rats were anesthetized with 20% chloral hydrate, and the bilateral common carotid arteries were isolated while the vertebral arteries were cauterized. On the second day after surgery, the rats underwent bilateral carotid artery ligation for 15 min. The Shame surgery group underwent the same procedures as the experimental group but without carotid artery ligation. During ischemia, the rectal temperature was maintained between 36.5°C and 37.5°C, and the ear temperature was maintained at 37°C.
Electrodes were pre-implanted on the skull of the rats prior to ischemia, positioned at the intersection of the coronal suture, with a depth reaching the brain surface. These electrodes served as the measurement and reference electrodes. Both electrodes were connected to a MacLab Bio Amp (ADInstruments Pty Ltd, Bella Vista, NSW, Australia) to record cortical electrical activity. After ischemia, all rats were placed in an incubator for 3 h (30°C–33°C) and then returned to their cages. The rats were randomly divided into 3 groups using a random number table: Shame surgery group (Shame), ischemia-reperfusion group (1/R), and ischemia-reperfusion + environmental enrichment intervention group (1/R + EEI), with 10 rats in each group.
A total of 30 male SD rats were randomly assigned to the following 3 groups (10 rats per group):
Shame surgery group (Shame): The SD rats underwent cauterization of the vertebral arteries without carotid artery ligation and were placed in standard housing conditions for one month.
1/R: SD rats that underwent the 4-VO ischemiareperfusion model were placed in standard housing conditions for one month.
1/R + EEI: SD rats that underwent the 4-VO ischemiareperfusion model were placed in an enriched environment for one month.
Shame surgery group (Shame) and 1/R: The housing conditions were set at an environmental temperature of 18°C–22°C, relative humidity of 50%–60%, with ad libitum food and water, and a balanced light–dark cycle. 1/R + EEI: Rats subjected to global cerebral ischemia and reperfusion were housed in spacious cages. The cages were equipped with nesting houses, climbing ladders, ropes, and chewable wooden pieces. In addition to providing sufficient water and food, peanuts and sunflower seeds were also offered. Music was played for 1 h at fixed times in the morning and afternoon, with the music type being soft classical music (e.g. Bach, Beethoven), the volume set at 60–70 dB, and the frequency of play being twice daily. The temperature around the cages was maintained between 18°C and 22°C, with a relative humidity of 50%–60%.
The depressive behavior of the SD rats was monitored on days 3, 14, and 28 post-modeling. The OFT and sucrose consumption test were used to monitor depressive behaviors, as they minimally affect the physiology of the animals.
To study the relationship between sucrose preference and depressive behavior in rats, the experiment was divided into an adaptation phase and a formal testing phase.10 During the adaptation phase, each rat was individually housed in a separate cage with 2 water bottles, one containing 1% sucrose solution and the other containing plain water. The positions and heights of the bottles were kept consistent, and the bottles were swapped every 12 h to ensure adaptation to changes in bottle placement. After the adaptation phase, the formal experimental phase began, during which sucrose solution and water were provided in sufficient amounts, and the initial weights of the bottles were recorded. After 24 h, the remaining sucrose and water volumes were measured. The sucrose preference was calculated as the ratio of sucrose consumed to the total volume of both sucrose solution and water. This preference serves as an indirect indicator of the rat’s depressive state, with depressed rats typically showing a lower sucrose preference, indicating reduced interest and activity.
The OFT is commonly used to assess rats’ emotional and behavioral responses, particularly anxiety and depression.11 The rat was placed in a large, open arena (100 cm × 100 cm × 40 cm), with marked areas to facilitate behavioral analysis. The rat was allowed to acclimatize briefly before being placed in the center of the arena for observation, with the experimental duration typically ranging from 5 min to 30 min. Observational measures included the total activity level (number of steps or total distance traveled), the time spent in the center versus the edges of the arena, and the number of line crossings. Depressive behavior was typically indicated by reduced activity in the center area, with the rat spending more time in the perimeter and showing decreased exploration and activity. These behavioral changes are used to evaluate depressive states, and the OFT is widely used for studying anxiety and depression in rats, as well as the effects of pharmacological interventions.
After data collection, the data will be coded and analyzed without disclosing the specific information of each group to the analysts. Statistical analysis was performed using GraphPad Prism 5.0 software (GraphPad Software, San Diego, CA, USA). Data are presented as mean ± standard deviation. All experiments were repeated 3 times to ensure the reliability and stability of the results. One-way analysis of variance (ANOVA) was used to compare differences in sucrose preference and central zone activity between the different groups (Shame, 1/R, 1/R + EEI). Data measurements within each group were independent, and the assumptions of one-way ANOVA were met. For the behavioral data, time was considered as a within-group factor, and treatment was a between-group factor. Statistical significance was set at P < 0.05.
In the sucrose consumption test, on the third day postischemia, there was no significant difference in sucrose preference between the 1/R group, 1/R + EEI group, and the Shame group (P > 0.05). However, on the 7th and 14th days post-ischemia, the sucrose preference in the 1/R group was significantly lower than that in the Shame group (P < 0.05). Compared to the 1/R group, the sucrose preference in the 1/R + EEI group was significantly higher (P < 0.05), as shown in Table 1 and Figure 1.
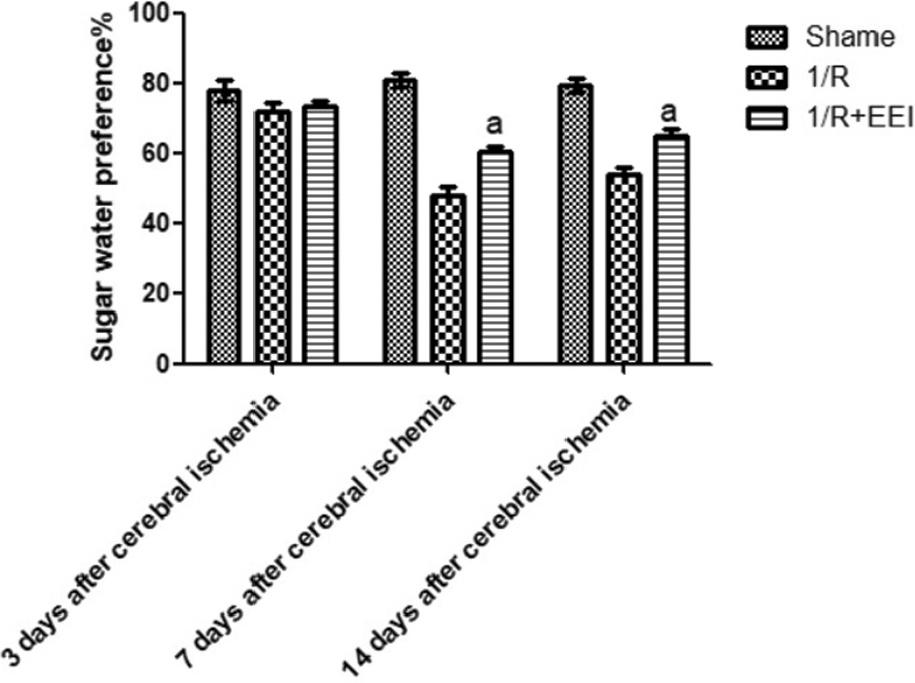
Sugar water preference. 1/R, ischemia-reperfusion group; 1/R + EEI, ischemia-reperfusion group + environmental enrichment intervention group.
Sugar water preference.
| Time groups | 3 d after cerebral ischemia | 7 d after cerebral ischemia | 14 d after cerebral ischemia |
|---|---|---|---|
| Shame | 78.00 ± 3.00 | 81.00 ± 2.00 | 79.33 ± 2.08 |
| 1/R | 71.67 ± 2.65 | 47.67 ± 2.52 | 54.00 ± 1.73 |
| 1/R + EEI | 73.33 ± 1.53 | 60.33 ± 1.53 | 64.33 ± 2.89 |
Note: 1/R, ischemia-reperfusion group; 1/R + EEI, ischemia-reperfusion group + environmental enrichment intervention group.
In the OFT, on the third day post-ischemia, there were no significant differences in the central zone activity distance between the Shame group, 1/R group, and 1/R + EEI group (P > 0.05). However, on the 7th and 14th days post-ischemia, the central zone activity distance in the 1/R group was significantly lower than that in the Shame group (P < 0.05). Compared to the 1/R group, the central zone activity distance in the 1/R + EEI group significantly increased (P < 0.05), as shown in Table 2 and Figure 2.
Distance to the central area of the open field.
| Time groups | 3 d after cerebral ischemia | 7 d after cerebral ischemia | 14 d after cerebral ischemia |
|---|---|---|---|
| Shame | 1743.33 ± 33.00 | 1753.33 ± 44.93 | 1740.00 ± 29.44 |
| 1/R | 1623.33 ± 47.84 | 753.33 ± 41.10 | 736.67 ± 33.00 |
| 1/R + EEI | 1726.67 ± 41.10 | 1073.33 ± 52.70 | 1100.00 ± 90.92 |
Note: 1/R, ischemia-reperfusion group; 1/R + EEI, ischemia-reperfusion group + environmental enrichment intervention group.
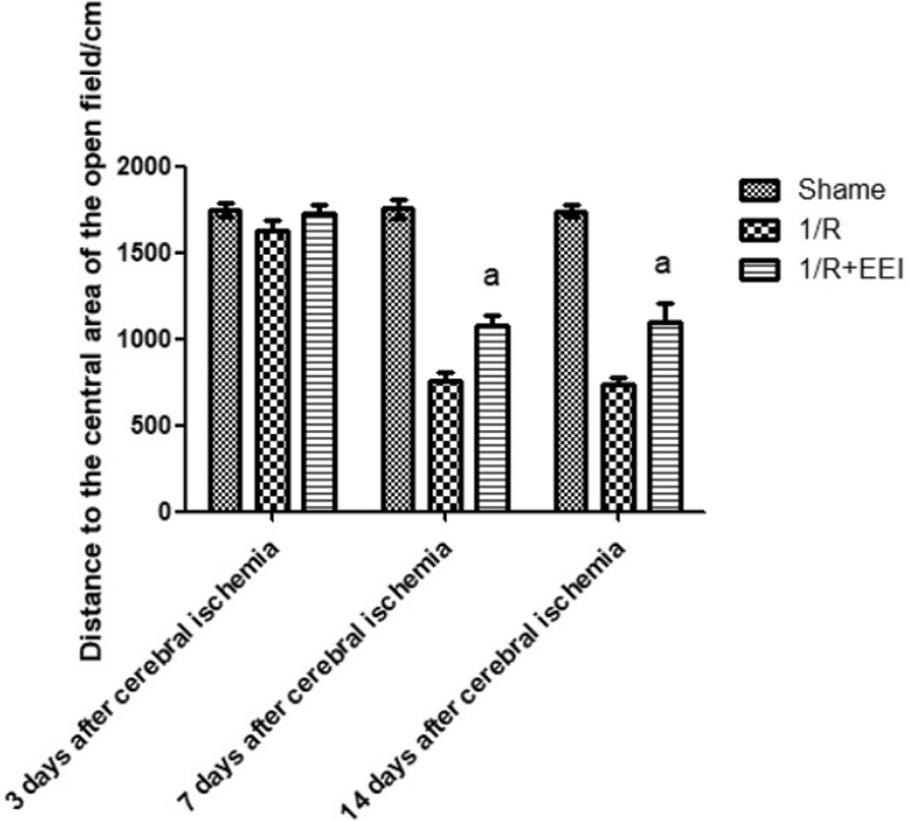
Distance to the central area of the open field. 1/R, ischemiareperfusion group; 1/R + EEI, ischemia-reperfusion group + environmental enrichment intervention group.
This study intervened in the depressive behavior of ischemic stroke rats through environmental enrichment, using behavioral assessment methods such as the sucrose consumption test and OFT, and verified the positive effect of environmental enrichment in alleviating post-stroke depressive symptoms. The results showed that environmental enrichment significantly improved depressive-like behaviors in ischemic stroke rats, as evidenced by increased sucrose consumption and restored activity in the OFT. This finding supports the effective intervention of environmental factors on depressive behavior in rats, suggesting that environmental enrichment can significantly alleviate depression caused by ischemic stroke by improving emotional state and activity levels.
Although significant improvements in sucrose consumption and central zone activity distance were observed on the 7th and 14th days post-ischemia, there were no significant differences in sucrose preference and central zone activity distance between the 1/R group and 1/R + EEI group on the third day postischemia. This phenomenon may be explained by the acute brain injury and neurophysiological responses during the acute phase of ischemic stroke. On day 3 post-ischemia, the rats’ neurological function and emotional state may still be in the acute response phase, and the brain’s neural damage has not yet stabilized or been fully repaired.
Therefore, during this phase, the rats’ behavioral performance may not show significant changes, and the effects of environmental enrichment intervention may not yet be fully manifested in the short term. Additionally, sucrose consumption and activity levels within the first 3 d may be influenced by multiple factors such as acute pain and fatigue, which may prevent a noticeable difference in depressive-like behavior. Brain-derived neurotrophic factor (BDNF) plays an important role in neuroplasticity and emotional regulation, but its expression typically requires some time to take effect. On the third day, it is likely that BDNF expression is still in its early stages, and its upregulation has not yet reached a level sufficient to induce significant behavioral changes. As a result, no significant differences were observed in the behavioral tests. Over time, BDNF expression may gradually increase, leading to more significant improvements in depressive behavior in the later stages. As time progresses and neurological function gradually recovers, the effects of environmental enrichment gradually become more evident, particularly on the 7th and 14th days post-ischemia, when sucrose consumption and central zone activity distance showed significant improvement. Certainly, the sample size in this study is relatively small, which introduces certain limitations. A small sample size may lead to less robust statistical analyses, which might not fully represent the true situation in larger sample sizes.
The innovation of this study lies in the introduction of the environmental enrichment concept into the nursing intervention for depressive behavior following ischemic stroke. It explored the efficacy of this intervention method for post-stroke depressive symptoms and provided new theoretical foundations and practical approaches for the psychological health intervention of ischemic stroke patients. Compared to traditional pharmacological interventions, environmental enrichment not only helps improve the rats’ emotional and behavioral responses but may also promote neural plasticity, providing new pathways for stroke recovery.
Based on the results of this study, it is suggested that, in the rehabilitation of ischemic stroke patients, in addition to traditional pharmacological treatments, environmental enrichment methods should be considered, such as providing rich social and environmental stimuli to promote psychological recovery and enhance quality of life. Moreover, clinical caregivers could explore combining environmental enrichment interventions with other non-pharmacological treatment methods (such as exercise therapy, cognitive behavioral therapy, etc.) to develop a more comprehensive rehabilitation model.
Future research could further explore the specific mechanisms of environmental enrichment interventions, especially how they improve depressive behaviors through neurobiological and psychological pathways. Additionally, clinical translational research could be conducted to verify the application and feasibility of environmental enrichment interventions in ischemic stroke patients, exploring their long-term effects on neuropsychiatric symptoms, particularly in improving quality of life and promoting neurological recovery. Furthermore, the optimization and individualization of environmental enrichment interventions should be an important direction for future research to better meet the needs of different patients.
In conclusion, environmental enrichment intervention, as a noninvasive and low-cost therapeutic approach, has broad application prospects, especially in the management of depressive symptoms in ischemic stroke patients. It holds the potential to provide new treatment strategies for clinical practice.