
Heart failure (HF) is defined by the American College of Cardiology (ACC) and the American Heart Association (AHA) as: “HF is a complex clinical syndrome that can result from any structural or functional cardiac disorder that impairs the ability of the ventricle to fill with or eject blood.”1 HF is a life-threatening disorder, and it is associated with higher rates of morbidity and mortality. It is estimated that the worldwide prevalence of HF is >64 million.2 In developing countries such as India, the burden seems to be higher with an estimated prevalence of 1.3–4.6 million and an annual incidence of 0.5–1.8 million.3 The prevalence of HF increases with age; compared with the younger population, the risk of HF increases by multiple folds in the elderly population aged >65 years. The prevalence of HF among the elderly has increased in recent decades.4 The emergent epidemic of HF in the elderly is linked to a demographic shift caused by several factors, including increasing life expectancy and the survival of patients with ischemic heart disease.5
Along with the high rate of hospitalization, a major challenge in the treatment and management of HF is the high rate of hospital readmissions. It is estimated that almost 50% of the patients discharged after HF-related hospitalization are readmitted within 6 months.6,7 Only one-fourth of the rehospitalizations are due to HF reexacerbation, while in most of the cases they are not related to HF. The prominent reasons for readmission are comorbidities, non-adherence to medications and treatment plans, and other non-cardiovascular conditions.8 Such frequent hospital visits not only translate to poor clinical outcomes but also contribute considerably to the rising healthcare costs.9
HF has a significant lifetime risk with poor prognosis, particularly following hospitalization. Despite substantial advancements in treatment over the past decades, patients with HF still face considerable risks, and the mortality rates remain high. It is therefore necessary to improve the management strategy and treatment planning for patients with HF.10,11 To achieve better results, there should be greater adherence to evidence-based management, and more human and material resources should be put in place to cater to the needs of patients with HF.12,13
Patients with HF often experience a myriad of physical and emotional problems which impact their daily physical and social activities, ultimately adversely affecting their quality of life (QoL).14 It has been demonstrated that QoL is a predictive factor of hospitalization, rehospitalization, and mortality rates. Poor QoL scores in patients with HF are associated with poor longterm prognosis and higher rates of hospitalization and mortality.15 Assessing the QoL is a vital tool that could help in identifying the risk as well as predicting the outcomes in patients with HF.16,17
Developed countries have gravitated toward effective management of HF with risk stratification, prevention, education, and treatment. However, owing to the lack of resources, poor monitoring, and information gathering, developing countries are still struggling to catch up.18 Understanding the local epidemiological characteristics, practice patterns, and patient-reported health-related QoL in patients with HF could provide pivotal information for preventive, curative, and public health strategies. The present study aims at comprehensively assessing the incidence of readmission, mortality, and QoL among patients with HF in a tertiary care hospital setting. It tries to provide nuanced insights into the challenges faced by patients with HF, enhancing the understanding for tailored interventions and improved patient outcomes.
A single-center, non-interventional, mixed-methods approach was used to evaluate the incidence of readmission, mortality, and QoL outcomes in patients with HF admitted to a tertiary care hospital in Karad, India. The study was conducted over a period of 24 months between November 2019 and October 2021. The study involved pre-discharge education, outpatient care, monthly telephonic follow-ups, and usual care. Followup assessments were done at 4 weeks, 6 months, and 12 months.
Patients aged ≥18 years diagnosed with ischemic and non-ischemic heart diseases with an ejection fraction (EF) <40%, and patients with chronic HF status and New York Heart Association (NYHA) class I–III symptoms were included in the study. Additionally, patients were required to be mentally alert and care for themselves, were literate, and had access to the telephone for communication. Preference was given to patients residing in close vicinity of the hospital.
Patients with dementia or any psychiatric illness, Cor-pulmonale, acute myocardial infarction, chronic renal failure, visual or auditory impairment, severe alcohol, or drug abuse were excluded. Patients with a planned surgical correction for HF within 12 months of being terminally ill with a life expectancy of <6 months were also excluded from the study.
Eligible patients were briefed about the study and enrolled after they provided a signed informed consent form. We accessed the patients’ medical records and history. Anonymized data were collected for the quantitative components, including date of first occurrence/diagnosis of HF, readmission date, reason for readmission, and the treatment outcomes. Baseline clinical assessments in patients with HF included the NYHA classification and Charlson comorbidity index. The patients were followed over a period of 2 years and the readmissions and mortality rates were calculated using this information. Mortality data was obtained by recording the discharge or death date and mentioning the status of discharge or death. The cause of death was recorded to identify frequent fatal complications. The number of days a patient spent in the hospital was also recorded to analyze the severity of the condition.
Complementing this, the qualitative aspect was captured using the QoL data of patients with HF using a standardized questionnaire of 21 questions. The aim of the questionnaire was to assess various aspects of daily life, including physical limitations (swelling, mobility, shortness of breath, etc.), social life, mental health, and the economic impact of the condition. The questionnaire was designed to address all possible challenges faced by HF patients. Patients were asked to circle the most appropriate response ranging from 0 to 5, to show how much their life was affected during the last month/4 weeks. A score of 0 meant no impact, whereas a score of 5 indicated a significant impact on their life. The questionnaire included questions to assess the impact on daily activities, including walking, climbing, independence in performing day-to-day activities, food habits, sleep, and sexual wellness. The questionnaire also assessed emotional wellbeing, including feeling of depression, burden on family/friends, and loss of selfcontrol. In addition, during the regular follow-up, we collected data in another questionnaire to understand the self-care pattern among patients with HF. The HF selfcare behavior scale comprised questions to analyze the behavior of patients with respect to self-care. It included questions related to daily exercise, appropriate dietary control, administration of medication, and reaching out to physicians in case of weight gain or symptoms of HF relapse. Patients or their representatives filled the questionnaires. If they were unable, the study coordinator asked the question verbally and recorded the patient’s response. In case of a challenge with in-person visit/follow-up, the patient responded to the questionnaire over a telephonic conversation. The data from the filled questionnaire were captured in an electronic master data sheet and then analyzed using statistical tools. Before analysis all patient-level data were anonymized.
All categorical data have been evaluated using descriptive statistics to calculate the proportion of patients who needed readmission, had an event of mortality, and QoL while living with HF. Multiple statistical tests such as the paired t-test, Chi square tests, and Pearson’s correlation were used to analyze the relationship between readmission rates, mortality, and living standards. A P value of <0.05 was considered statistically significant for all statistical tests. Data were collected in a master data sheet using Microsoft Excel. Data analysis was performed using the Statistical Packages for Social Sciences (SPSS) version 28.0 software (IBM Corp based in Chicago, IL, USA).
Pearson’s correlation coefficient was used to study the correlation between parameters. For the test–retest reliability coefficient, the measure was given to the same individuals at different times and how much the results varied over time was examined. The attribution classification and measurement reliability coefficient for the evaluation index was set as 0.785 for ensuring the quality of data collected. To assess the living standards, a standard of internal consistence of 0.778 was utilized, which was analyzed by Cronbach’s alpha—this was done to ascertain high reliability of the data collected.
The study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants before being enrolled in this study. The Institutional Ethical Committee approved the research protocol (KIMSDU/IEC/03/2018) before initiating the study. All patient-level data were anonymized so as to protect patients’ privacy.
A total of 98 patients who met the eligibility criteria were enrolled in the study. Table 1 provides a summary of the baseline demographics and disease characteristics of the enrolled patients. Most of the patients were male (63.3%) and aged ≥61 years (66.3%). Most of the patients (59.2%) had been diagnosed with HF recently (1–6 months). At the end of their treatment 75.5% of patients were discharged feeling improved or getting cured while 12.2% patients succumbed to HF during treatment.
Baseline demographics and disease characteristics (n = 98).
| Characteristics | Values, n (%) |
|---|---|
| Age (mean ± SD, years) | 62.9 ± 17.6 |
| Age range (years) | |
| 18–30 | 6 (6.1) |
| 31–45 | 6 (6.1) |
| 46–60 | 21 (21.4) |
| 61–75 | 50 (51.0) |
| >75 | 15 (15.3) |
| Gender | |
| Male | 62 (63.3) |
| Female | 36 (36.7) |
| Time since diagnosis of HF (months) | |
| <1 | 5 (5.1) |
| 1–6 | 58 (59.2) |
| 6–12 | 26 (26.5) |
| 12–36 | 9 (9.2) |
| No of days of hospitalization | |
| 1–10 | 65 (66.3) |
| 10–15 | 14 (14.3) |
| 16–30 | 8 (8.2) |
| 31–35 | 0 |
| 36–60 | 8 (8.2) |
| >60 | 3 (3.1) |
| Condition at discharge | |
| Cured | 30 (30.6) |
| LAMA/DAMA | 12 (12.2) |
| Improved | 44 (44.9) |
| Death | 12 (12.2) |
| Education | |
| Secondary | 42 (42.9) |
| Higher secondary | 39 (39.8) |
| Undergraduate | 15 (15.3) |
| Occupation | |
| Farmer | 21 (21.4) |
| Housework | 20 (20.4) |
| Not working | 44 (44.9) |
| Private employee | 13 (13.3) |
Note: DAMA, discharge against medical advice; HF, heart failure; LAMA, left against medical advice; SD, standard deviation.
Nearly 81% of the patients were admitted for <15 days while 3 patients required a stay of >60 days.
The rate of rehospitalization/readmission was 24.4%; 21.4% did not require readmission. Almost half of the patients (49%) were unable to come for a follow-up to the hospital because of the coronavirus disease 2019 (COVID-19) pandemic, while 5.1% patients went to a nearby physician/cardiologist outside the tertiary care hospital setting.
Over the 24-month study duration, the mortality rate was 43.9% and 43 patients succumbed to death because of HF and related complications. It is important to note that 28 (28.6%) patients had contacted COVID-19, and it could have exacerbated HF and related complications in some patients.
Based on the patient response for the self-care questionnaire, 54% of patients were taking mild care, while nearly 45% of the patients were taking average care of themselves. Only one patient seemed to be taking good care after being diagnosed with HF. Nearly 60% of the patients did not check their weight or exercise regularly. Details of the response to the self-care behavior questionnaire are summarized in Figure 1.
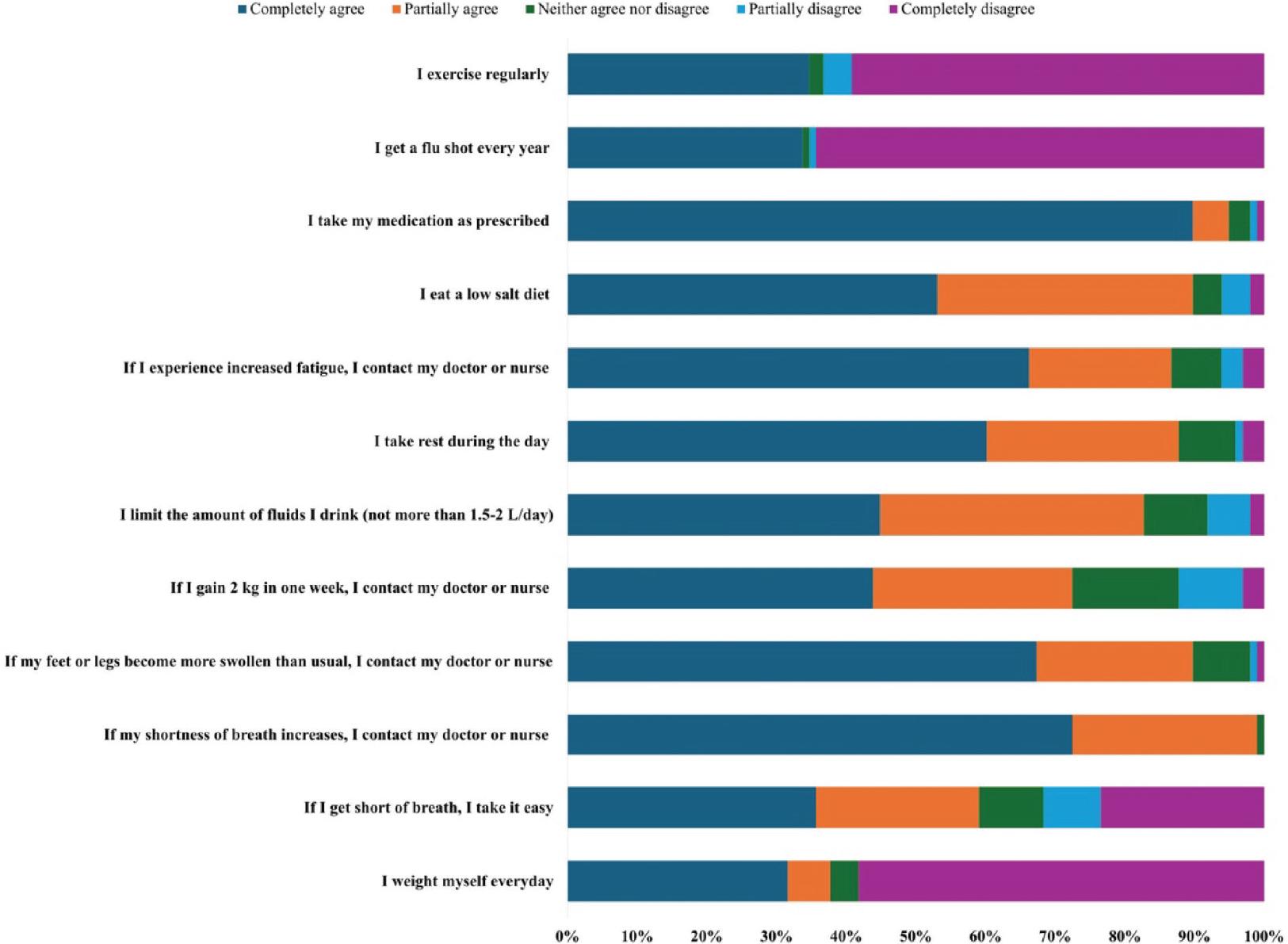
Patient response to self-care behavior questionnaire.
The patient-reported QoL data revealed that 22 (22.4%) patients felt that their QoL was good despite having HF, while 44 (44.9%) patients felt that they were living an average life due to HF. Thirty-two (32.7%) patients experienced an impact of HF and felt that they were struggling and had a low-quality life. Details of response provided by the patients for the 21 question QoL questionnaire are presented in Figure 2. Nearly 41% of patients had trouble in performing daily activities such as walking, climbing stairs, and working around the house or yard, while 49% patients experienced difficulty in going to places away from their home. HF impacted the sleep pattern and approximately 94% patients experienced little to very high difficulty in sleeping well at night. Nearly 46% of patients felt that due to HF they were experiencing medium to a very high level of difficulty in relating to or doing things with friends or family as well as in recreational activities, sports, or hobbies. More than 90% of patients were experiencing short breath and felt tired, fatigued, or low on energy. HF impacted sexual wellness in 68.4% patients as they experienced little to great difficulty in sexual activities; 67.4% of patients felt they were eating less of the foods they liked because of HF. About 83% of patients reported little to much difficulty in working to earn a living. HF impacted the mental wellbeing of patients, and nearly 74% of patients experienced little to much difficulty in concentrating and remembering things. Living with HF made patients feel that they were a burden on their family and friends (65.2%) and nearly 80% of patients felt they had lost control of their life. While 76.4% mentioned that they experienced little to very high worry, nearly 78% patients reported that they experienced little to very high depression due to HF.
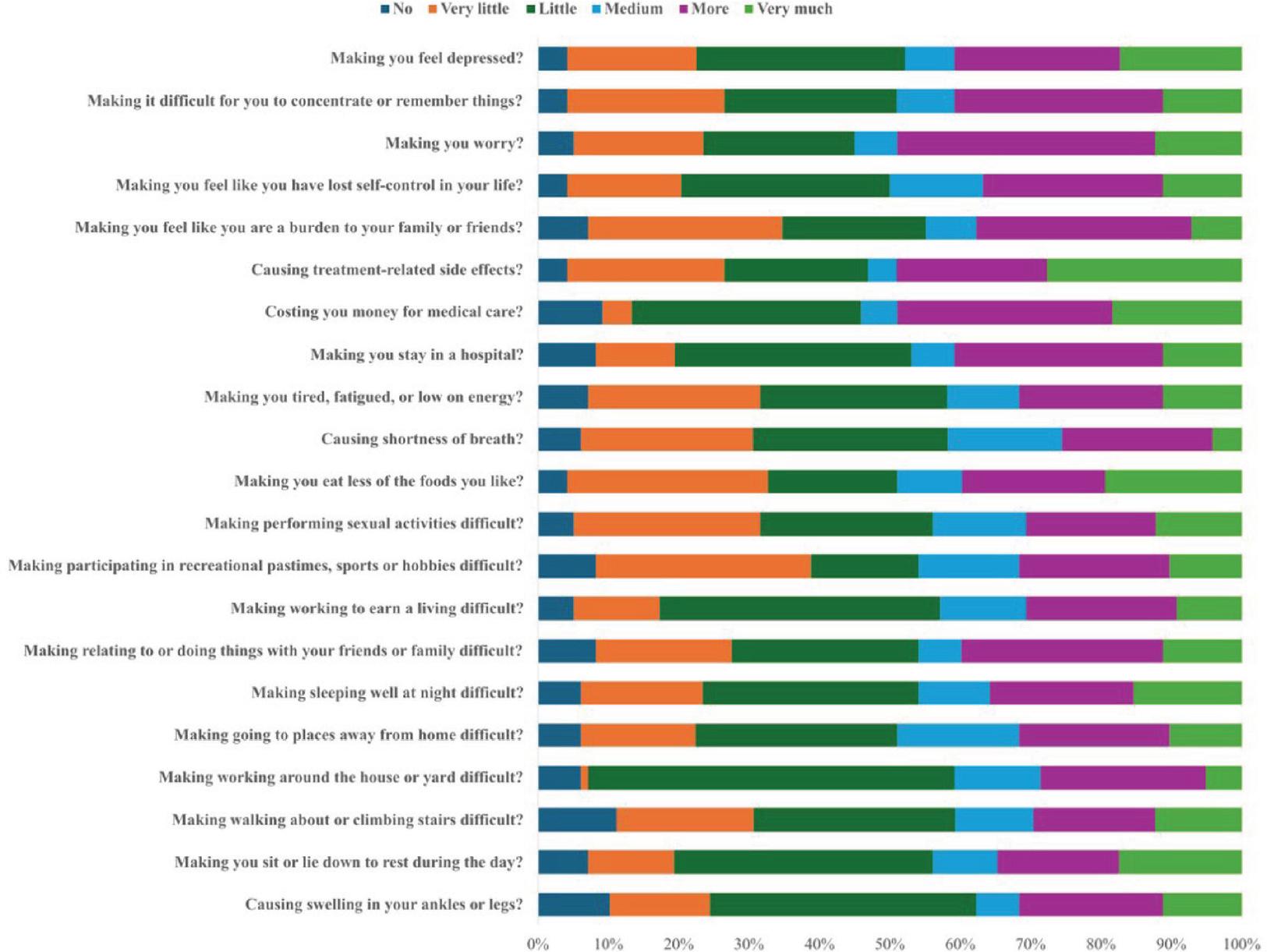
Patient response to 21-question QoL questionnaire. Note: QoL, quality of life.
Well-educated patients were more likely to understand the importance of and practice self-care compared with less educated patients (P = 0.001). Patients practicing better self-care were less likely to be readmitted (χ2 = 13.81, P < 0.05). Unemployed patients were more likely to experience average living conditions due to HF (P = 0.003).
In the present study, we were able to assess the data on incidence of readmission, mortality, and QoL of 98 patients with HF in a tertiary care hospital setting in Karad, India. The study findings revealed that one-fourth of the patients with HF required readmission, whereas nearly one-fifth of them did not require readmission. We observed a higher mortality rate compared with what is reported in the literature. Although the reason behind this increase could not be identified, the COVID-19 pandemic could have been a contributing factor for this unexpected outcome. One third of the patients with HF experienced a major impact of HF on their QoL. The QoL data showed that HF not only impacts the patients physically, but it also impacts their emotional and psychological wellbeing. Our study provides important insights into readmission, mortality, and the impact of HF on patients’ wellbeing and daily activities.
Compared with the younger population, elders aged ≥60 years have a 20-fold higher risk of developing HF (P < 0.001).4 The prevalence rates rise from 1% in individuals aged <50 years to over 10% in individuals aged >80 years.19 Ohlsson et al.20 assessed 3874 participants, in which 68% were male and the median age was found to be 57 years. Even in our study, the prevalence was higher among patients aged ≥61 years compared with those aged between 18 years and 45 years (66.3% vs 12.24%). We also noted the preponderance of males, as 62 (63.3%) patients enrolled in our study were male. Desai et al.21 have reported that male farmers are at an elevated risk of developing HF than other occupations. Even in our study, 21% patients with HF were farmers and male.
In a study that assessed the length of stay in hospital in 385 patients with HF, it was observed that most of the patients were hospitalized for 6–10 days.22 The results from our study align with the data reported in the existing literature: 65 (66.3%) patients were hospitalized for <10 days while 79 (80.6%) patients were hospitalized for <15 days.
A systematic review and meta-analysis by Foroutan et al.23 analyzed the readmission rates in 1.5 million individuals at risk. The proportion of patients readmitted in 30 days was 13.2%, while 35.7% were readmitted within 1 year. The 30-day and 1-year mortality rates were 7.6% and 23.3%, respectively. In another systematic review and meta-analysis by Lan et al.24 the 30-day and 1-year all-cause readmission rates were 19% and 53%, respectively. The 30-day and 1-year all-cause mortality rates were found to be 14% and 29%, respectively. The study also found that comorbidities were highly prevalent among individuals with HF. In our study, the 2-year readmission and mortality rates were 25% and 43%, respectively. These rates were higher compared with those reported in the published literature. We were unable to pinpoint a specific reason for this anomaly. However, a considerable number of patients were impacted by COVID-19, and it might have impacted the survival rates.
COVID-19 resulted in inaccessibility of the study sites and in-person scheduled study visits and/or followup. The rapid emergence and widespread effects of COVID-19 impacted on the management of clinical trials and research.25 It is important to note that myocardial injury was observed in ≥10% of COVID-19 cases, and up to 41% in critically ill patients or those with cardiovascular comorbidities. Some cases of COVID-19-related acute myocarditis, characterized by severe reduction in left ventricular EF and unique histopathological features, have been reported. Recent studies indicate that COVID-19 may be linked to both systolic and diastolic left ventricular dysfunction, with diastolic dysfunction, pulmonary hypertension, and right ventricular dysfunction being the most common echocardiographic findings.26 Considering the above facts, we feel that COVID-19 might have resulted in increased readmission and mortality rates in our study.
Johansson et al.27 analyzed factors affecting health-related QoL in 23,000 patients with HF from 40 countries. The results indicate that most participants experienced a poor QoL. Mulugeta et al.28 used the Minnesota Living with Heart Failure Questionnaire (MLHFQ) to assess the impact of HF on health-related QoL. They found that more than half of the patients (54%) experienced a poor QoL. In our study, 32.7% of patients with HF reported a poor QoL, while nearly 45% of patients felt it was average. It is already established that a lower QoL in patients with HF is associated with an increased risk of rehospitalization and mortality.29 In our study, 32 patients (32.65%) reported a low standard of living, and 24% had readmission. Our study results corroborate with the outcomes reported in the existing literature.
By enabling patients to better maintain their health, better patient education and self-care can substantially reduce the readmission and mortality rates. Patients can avoid difficulties and promote proactive health management by being informed about their disease, treatment plan, and the significance of adherence to medication. Personalized educational materials, phone or remote follow-up support, teaching self-monitoring skills, and encouraging dietary and exercise improvements are some of the suggested therapeutic strategies. Furthermore, support by nurses, healthcare providers, and family members in the teaching process can improve patient comprehension and compliance, which will ultimately lower the risk of readmission and improve long-term health outcomes.30–32
There are limitations in single-center observational studies and our study too had some limitations. Being a single-center observational study, patient characteristics could be influenced by the demographics of this region. The number of patients included was small and therefore, the results could not be generalized. Moreover, the practice pattern of the hospital could have influenced the study outcomes. Nearly half of the participants were unable to visit the hospital due to the COVID-19 pandemic, this impacted and influenced the study data. However, irrespective of the limitations, this study provides valuable information regarding patients with HF in this region.
To summarize, this study provides important data regarding the readmission, mortality, and QoL in patients with HF in and around Karad, India. It further strengthens the fact that HF impacts patients’ overall well-being. Although the mortality rate was high, we cannot pinpoint the reason behind it. The emergence of the COVID-19 pandemic disrupted the follow-up schedule and reduced the sample size, thus increasing the number of fatalities. It is well-known that patients with a lower QoL have higher readmission and mortality rates and the results from our study further substantiated this fact. The results suggest that along with physical health, HF impacts mental, psychological, and even the socioeconomic conditions of patients. Large multicenter studies with a larger patient population will help in demystifying the impact of pandemic on HF care, and the role of mental health and socioeconomic perspectives in QOL.