
An increased risk of dental caries is a recognised adverse effect of orthodontic treatment. A recent study identified the incidence of white spot lesion (WSL) development during removable aligner treatment as 1.2%, and 26% with fixed appliances. 1 The presence of orthodontic appliances creates niches for biofilms to develop and persist. In the presence of a cariogenic diet, undisturbed biofilms lead to an ecological shift and the creation of an acidic environment resulting in demineralisation and the development of carious lesions. 2 Incipient carious lesions present clinically as opaque WSLs. Untreated WSLs may progress to irreversible tooth destruction, which necessitates restorative management with on-going maintenance, significant costs and future disease burdens. 3
Three meta-analyses (MA) and seven systematic reviews (SR) have been conducted to investigate the preventive effects of various interventions. 4-13 The reports investigated fluoride (F), chlorhexidine (CHX), and casein phosphopeptide amorphous calcium phosphate (CPP-ACP). However, split mouth studies contributed to 50% of the quantitative analysis presented in one MA. 11 These studies were significantly confounded due to carry-across effects, which produced bias in treatment efficacy estimates. 14,15 Additionally, there were no statistical tests to detect the carry-across effect. 15 Two SRs investigated post-orthodontic WSL inhibition, rather than prevention, which is the focus of the present SR. 10,13 Two SRs included non-randomised controlled trials (RCTs), and one did not conduct a risk of bias assessment, which significantly affected their internal validity. 6,7,12 A Cochrane review identified the need for measuring treatment effect over the entire duration of orthodontic treatment, to prevent an overestimation of efficacy. 5 However, this review investigated the effects of F alone, and could not perform meta-analyses. Additional analyses comparing short- and long-term effects were lacking in another SR. 9
Moreover, recent preventive interventions such as self-assembling peptides (SAPs) have not been investigated within SRs. SAPs putatively show promising remineralisation effects by providing a template for mineral precipitation, but evidence is limited. 16-18
Therefore, the present systematic review aimed to assess and compare the preventive effects of various emerging and conventional interventions aimed to prevent WSLs during fixed and removable orthodontic care.
The review protocol was devised a priori and registered in the International Prospective Register of Systematic Reviews (PROSPERO; CRD42019137627).
The PICO framework was:
Participants: Orthodontic patients undergoing fixed or removable orthodontic treatment, without age or gender restrictions.
Interventions:
-
Topical F: toothpaste/dentifrice, mouth rinse, gel, and varnish. The following formulations were included: sodium fluoride (NaF), sodium monofluorophosphate (SMFP), stannous fluoride (SnF2), acidulated phosphate fluoride (APF) and amine fluoride (AmF).
-
F releasing adhesives and elastomeric ligatures.
-
Products containing CHX, CPP-ACP and CPP-ACPF.
-
Other calcium products: tricalcium phosphate (TCP) and nano-hydroxyapatite.
-
Resin modified glass ionomer cement (RMGIC) coating.
-
SAP.
-
Oral hygiene and dietary modifications.
Comparison: Either placebo or another treatment.
Outcomes: The primary outcomes were incidence of WSLs and their inhibition (arrest and/or reversal), as measured using either ICDAS or DMFT. The total number of carious lesions at the end compared to the start of the study was utilised to obtain a risk ratio.
The secondary outcomes included differences in lesion size between control and intervention groups. This was measured at the end of the study, using quantitative light induced fluorescence (QLF). Self-reports of adverse events, side-effects and tolerability were also recorded.
For binary outcomes (absence or presence of WSLs), the relative risk (RR) was computed at 95% confidence intervals (CI). For continuous data (change in mean scores of WSLs from start to end of the study), the mean difference was calculated at 95% CI.
English language RCTs in humans from 1970 to June 2019, with a duration of at least six months, were included. Exclusion criteria were non-randomised designs, laboratory-based (in vitro, in vivo and ex vivo), retrospective, split mouth studies and trials that did not record WSLs at the onset and at the end of treatment. Post-orthodontic WSL inhibition studies were also excluded.
A systematic search of Embase, MEDLINE and Cochrane Central Register of Controlled Trials (CENTRAL) was performed. The search strategy is provided in Supplementary Table I. Unpublished studies were sought by searching ClinicalTrials.gov. The reference lists of included papers were hand searched to screen for relevant studies.
MEDLINE OVID search strategy.
| Search key words | |
|---|---|
| 1 | Prevent* |
| 2 | Fluoride* or toothpaste* or tooth paste or mouthrinse* or mouth rinse* or mouth wash* or gel or varnish or NaF or SMFP |
| or SnF or APF or amine F or f releas* or dentrific* | |
| 3 | tooth brushing or dental devices, home care/ |
| 4 | Exp cariostatic agents/or cariostatic |
| 5 | Chlorhexidine or chlor hexidine |
| 6 | CPP ACP or casein phosphopeptide amorphous calcium phosphate |
| 7 | RMGI or resin modified glass ionomer* |
| 8 | SAP or self assembling peptide* |
| 9 | Oral hygiene or OHI |
| 10 | Or/1-9 |
| 11 | caries or incipient lesion* or WSL or cavity or cavities or white spot |
| 12 | demineralization or demineralisation |
| 13 | or/11-12 |
| 14 | fixed or orthodont* or brace* or edgewise or begg |
| 15 | removable or removed or appliance* |
| 16 | exp orthodontics/ |
| 17 | or/14 -16 |
| 18 | 10 AND 13 AND 17 |
| 19 | randomized controlled trial.pt |
| 20 | controlled clinical trial.pt |
| 21 | random* or blind* |
| 22 | trial or trials |
| 23 | or/19 – 22 |
| 24 | 18 AND 23 |
| 25 | limit 24 to English language |
Following the removal of duplicates, the titles and abstracts were screened for inclusion. Relevant articles had their full texts assessed to determine suitability for inclusion or exclusion. The study selection was done independently by two authors (JM and MS) (Figure 1). A third author (DM) was contacted to confirm the randomisation process in older studies.
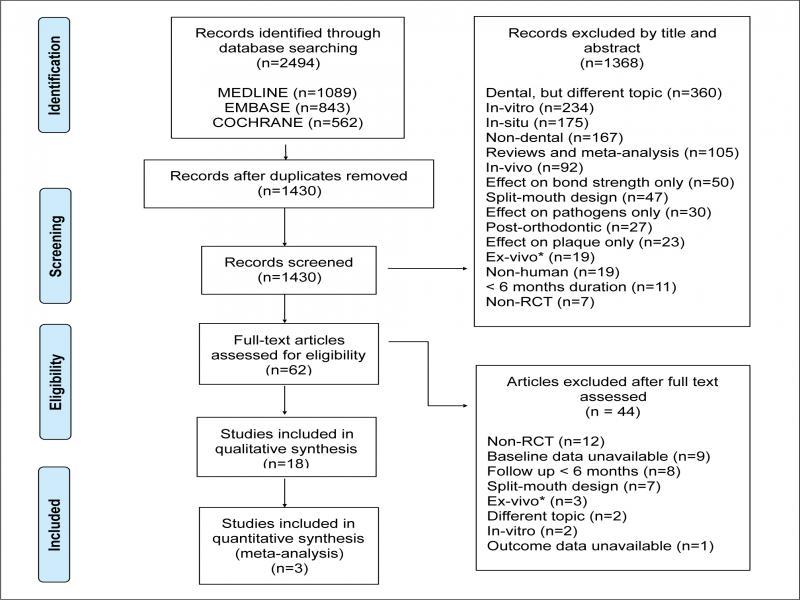
PRISMA flowchart presenting the study selection and identification process.
Data extraction was performed by the first author (JM) using Excel (Microsoft, 2019, Chicago), and audited by MS. Disagreements were resolved by discussion with DM. Data items included sample size, age of participants, intervention, comparison, frequency of intervention, follow-up period, outcome measure, baseline and outcome data. When required, authors were contacted via email correspondence for clarification of missing data.
The Cochrane RoB 2 tool was used to evaluate bias in the included RCTs. 19 This tool evaluates bias across five domains: the randomisation process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result.
Statistical heterogeneity was assessed by the I2 statistic, with significance set at p < 0.05. These statistical analyses and meta-analysis were performed using Jamovi (an open statistical software) with a random-effects model, due to expected heterogeneity. 20
Following NHMRC recommendations, GRADE was used to determine the quality of evidence, to facilitate the development of a clinical guideline for the prevention of WSLs during orthodontic treatment. 21 Publication bias was planned for assessment using funnel plots, if more than 10 studies were included in the quantitative analysis. Subgroup analyses for age, gender, preventive measure, outcome measure and type of appliance were planned.
A total of 2494 citations were identified through the searches. Following duplicate removal, 1430 articles were available for title and abstract screening. This led to the exclusion of 1368 studies. Subsequently, 62 articles had their full texts read. Based on the predetermined inclusion/exclusion criteria, 44 articles were excluded (Supplementary Table II), and 18 RCTs were included in the qualitative analysis. Following the risk of bias assessment, three RCTs were pooled for quantitative synthesis. The study selection process is illustrated in Figure 1.
Reasons for exclusion following full-text assessment.
| Study | Reason for exclusion |
|---|---|
| Dimitriadis AG, Sassouni V, and Draus FJ (1974). | Non randomised |
| Boyd RL (1992). | Non randomised |
| Boyd RL (1993). | Non randomised |
| Turner PJ (1993). | Non randomised |
| Banks PA and Richmond S (1994). | Split mouth |
| Boyd RL and Rose CM (1994). | Non randomised |
| Silverman E, Cohen M, Demke RS, and Silverman M (1995). | Non randomised |
| Trimpeneers LM and Dermaut LR (1996). | Non randomised |
| Marini I, Pellicioni GA, Vecchiet F, Bonetti GA, Checchi L. (1999). | Baseline data not available |
| Wenderoth CJ, Weinstein M, and Borislow AJ (1999). | Split mouth |
| Banks PA, Chadwick SM, Asher-McDade C, Wright JL (2000). | Baseline data not available |
| Hsu CYS, Jordan TH, Dederich DN, and Wefel JS (2000). | Non randomised |
| Harazaki M, Hayakawa K, Fukui T, Isshiki Y, and Powell LG (2001). | Non randomised |
| Ogaard B, Larsson E, Henriksson T, Birkhed D, and Bishara SE (2001). | Baseline data not available |
| Donly KJ (2003). | Ex-vivo |
| Zimmer BW and Rottwinkel Y (2004). | Non randomised |
| Abdullah AZ, Stafford SM, Brookes SJ, and Duggal MS (2006). | In-vitro |
| Miura KK, Ito IY, Enoki C, Elias AM, and Matsumoto MAN (2007). | < 6 months |
| Shafi I (2008). | Non-randomised |
| Dong YN, Chen M, and Ren XM (2009). | Split mouth |
| Tenuta LMA, Zamataro CB, Del Bel Cury AA, Tabchoury CPM, and Cury JA (2009). | Split mouth |
| Akkurt MD, Amasyali M, Ozcan S, Yagci A, Basak F, and Sagdic D (2011). | < 6 months |
| Buck T, Pellegrini P, Sauerwein R, Leo MC, Covell Jr DA, Maier T, and Machida CA (2011). | Split mouth |
| Demito CF, Rodrigues GV, Ramos AL, and Bowman SJ (2011). | Split mouth |
| Najibfard K, Chedjieu I, Ramalingam K, and Amaechi BT (2011). | < 6 months |
| Stafford GL (2011). | Non-randomised |
| Sollenius O, Karlsson L, Petersson LG, and Twetman S (2013). | < 6 months |
| Atwa ALDA,. AbuShahba RY, Mostafa M, and Hashem MI (2014). | < 6 months |
| Melo MA, Morais WA, Passos VF, Lima JP, and Rodrigues LK (2014). | In-vitro |
| Ghajari MF, Eslamian L, Rad AN, and Morovati SP (2015). | Baseline data not available |
| Masoud MI, Allarakia R, Alamoudi NM, Nalliah R, and Allareddy V (2015). | Outcome data not available |
| Paschoal MA, Moura CMZ, Jeremias F, Souza JF, Bagnato VS, Giusti JSM, and Santos-Pinto L (2015). | < 6 months |
| Restrepo M, Bussaneli DG, Jeremias F, Cordeiro RCL, Magalhaes AC, Palomari Spolidorio DM, and Santos-Pinto L (2015). | Ex-vivo |
| Zhang N, Chen C, Weir MD, Bai Y, and Xu HH (2015). | Ex-vivo |
| Bussaneli DG, Jeremias F, Cordeiro RC, Raveli DB, Magalhaes AC, Candolo C, and Santos-Pinto L (2016). | < 6 months |
| Gizani S, Petsi G, Twetman S, Caroni C, Makou M, Papagianoulis L (2016). | Baseline data not available |
| Hammad S and Abdellatif A (2016). | Baseline data not available |
| Miller CC, Burnside G, Higham SM, Flannigan NL (2016). | Baseline data not available |
| Oosterkamp BCM, Wafae A, Schols JGJH, van der Sanden WJM, and Wensing M (2016). | Different topic |
| Korkmaz YN and Yagci A (2018). | < 6 months |
| Liptak L, Szabo K, Nagy G, Marton S, and Madlena M (2018). | Split mouth |
| Benson PE, Alexander-Abt J, Cotter S, Dyer F, Fenesha F, Patel A, Campbell C, Crowley N & Millett D (2019). | Baseline data not available |
| Enerback H, Moller M, Nylen C, Odman Bresin C, Ostman Ros I, and Westerlund A (2019). | Different topic |
| Sonesson M, Brechter A, Abdulraheem S, Lindman R, Twetman S (2019). | Baseline data not available |
The characteristics of the 18 RCTs included in the qualitative analysis are summarised in Supplementary Table III. Ten trials investigated F, three assessed CHX, two CPP-ACP, two oral hygiene, and one assessed laser intervention. 22-39
Data from studies included in the qualitative synthesis.
| Study (year, country) | Sample size | Age of participants | Intervention | Control/Comparison |
|---|---|---|---|---|
| Ogaard et al. (1997, Sweden) | 198 (101 experimental; 97 controls) | 12-15 | Fluoride varnish (Fluor Protector); Antimicrobial varnish (Cervitec) | Placebo and F varnish |
| Alexander et al. (2000, US) | 72 (22:25:25 – controls, 2*experimental groups) | Mean 13.93 | Group 1: Tooth brush instruction, high potency and frequency F gel; Group 2: Tooth brush instruction, high potency and frequency dentrifice | Tooth brush instruction, low potency, high frequency F rinse |
| Weiss et al. (2005, Germany) | 68 (34 per group) | Mean 14.1 | Chlorhexidine gel in chair and 2.26% NaF varnish | 40% chlorhexidine varnish and 2.26% NaF varnish |
| Al Mulla et al. (2010, Saudi Arabia) | 100 (51 experimentals; 49 controls) | Mean 16.9 | Modified F toothpaste technique: minimal rinsing of paste after brushing (1450 ppm F) | Regular brushing (1450 ppm F) |
| Hoffman et al. (2015, USA) | 48 (24 per group) | Mean 15.6 in experimental group 15.3 in control | 5000ppm NaF with 5% NovaMin paste | 1500ppm F toothpaste |
| Suetenkov et al. (2015, Russia) | 60 (30 per group) | 12-13. | Laser therapy (OPTODAN and FotoSan) with control goup regime | Twice daily brushing with 1400ppm F paste, 0.05% CHX mouthrinse for 10 days, F gel |
| Esenlik et al. (2016, Turkey) | 40 (20 per group) | Mean 17 | CPP-ACP paste | No treatment |
| Alavi et al. (2018, Iran) | 40 (10 in each group) | Mean 23 | Group 1: 0.2% CHX varnish; Group 2: 5% NaF varnish | Group 3: placebo varnish; Group 4: control |
| Gomeza et al. (2018, Spain) | 20 (10 per group) | Mean 15.0 in experimental group 14.2 in control | Photodynamic therapy – Methylene blue activated by laser at 670nm | Ultrasonic scaler clean |
| Janatschke et al. (2001, Germany) | 33 (18 experimentals; 15 controls) | Median 15 | 40% chlorhexidine varnish | Placebo |
| Ogaard et al. (2006, Sweden) | 97 (50 experimentals; 47 controls) | Mean 14.4 | AmF/SnF2 (1400ppm F) toothpaste and 250ppm F rinse | NaF (1400ppm F) toothpaste and 250ppm F rinse |
| Steckson-Blicks et al. (2007, Sweden) | 257 (132 experimentals; 125 controls) | 12-15. | F varnish (0.1% F) | Placebo varnish |
| Jiang et al. (2013, China) | 95 (48 experimentals; 47 controls) | 10-20. | 1.23% APF foam | Placebo foam |
| Fretty (2014, USA) | 55 | 13 | 1.23% APF foam | Placebo foam |
| Sonesson et al. (2014, Sweden) | 391 (188 experimentals; 192 controls) | 11-16. | 5000ppm NaF paste | 1450ppm NaF paste |
| van der Kaaij et al. (2015, Netherlands) | 81 (36 experimentals; 45 controls) | Mean 13.3 | 250ppm F rinse (100ppm AmF, 150ppm NaF) | Placebo rinse |
| Zotti et al. (2016, Italy) | 80 (40 per group) | Mean 14.1 in study group 13.6 in control | Whatsapp based reminder re OH | No app based reminders |
| Rechmann et al. (2018, USA) | 37 (19 experimentals, 18 controls) | Mean 15.9 | 1100ppm F paste with MI Varnish (10% w/v CPP-ACP, 5% NaF) and MI Paste Plus (10% w/v CPP-ACP, 0.2% 900ppm NaF) | 1100ppm F paste with 0.05% NaF rinse |
| Frequency | Follow up period | Outcome measure | Baseline | Outcome | Adverse effects |
|---|---|---|---|---|---|
| Pre-bonding, Cervitec: weekly for 3 weeks. F varnish applied at bonding. Cervitec 6 weeks later | Both varnishes: 3 monthly afterwards | 6 months | WSL index | Experimental – mean 1.1 SD 0.2; Control – mean 1.1 SD 0.1 | Experimental – mean 1.1 SD 0.2; Control – mean 1.1 SD 0.1 | None reported |
| Control: 2/day brushing with 1.1% NaF dentrifice and 0.05% APF rinse; Group 1: 2/day brushing with 1.1% NaF dentrifice and 1.1% NaF gel; Group 2: 2/day brushing with 1.1% NaF dentrifice | Group 1 – 27.1; Group 2 – 26.4; Control – 24.8 | Enamel Demineralisation Scale | Group 1 – 3.8 SD 5.8; Group 2 – 4.4 SD 6.8; Control – 2.1 SD 3.8 | Group 1 – 6.4 SD 10.4; Group 2 – 6.0 SD 9.2 ; Control – 10.2 SD 14.2 | None reported |
| CHX 3 monthly. F varnish 4 and 8 week rotations | 10 months | DMFS | Experimental – mean 10.9 SD 2.5; Control – mean 10.9 SD 4.5 | Experimental – mean 15.1 SD 4.5; Control – mean increase 14.4 SD 5.5 | None reported |
| Daily practice | 24 months | DFS | Experimental – mean 8.3 SD 7.5; Control – mean 8.1 SD 8.4 | Experimental – mean 9.0 SD 8.0; Control – mean 11.6 SD 10 | None reported |
| Daily practice | 6 months | Decalcification index | Experimental – mean 0.33 SD 0.34; Control – mean 0.33 SD 0.4 | Experimental – mean 0.47 SD 0.37; Control – mean 0.44 SD 0.47 | None reported |
| 3 monthly | 18 months | DMFS | Experimental – mean 3.33 SD 0.17; Control – mean 3.76 SD 0.33 | Experimental – mean 5.99 SD 0.19; Control – mean 5.13 SD 0.15 | None reported |
| Monthly | Debonding (25 months) | DMFT, DMFS, WSL Index | [WSL Index] Experimental – mean 0; Control – mean 0 | [WSL Index] Experimental – mean 1.9 SD 1.5; Control – mean 4.1 SD 4.0 | None reported |
| 3 monthly | 9 months | ICDAS | Group 1 – 1.5 SD 0.52; Group 2 – 1.4 SD 0.51; Group 3 – 1.1 SD 0.31; Group 4 – 1.1 SD 0.31 | Group 1 – 1.1 SD 0.00; Group 2 – 1.0 SD 0.00; Group 3 – 1.2 SD 0.63; Group 4 – 1.30 SD 0.48 | None reported |
| 2 weekly intially. Then three monthly | 9 months | ICDAS | Experimental – mean 0.14 SD 0.03; Control – mean 0.13 SD 0.02 | Experimental – mean 0.21 SD 0.025; Control – mean 0.2 SD 0.02 | None reported |
| 8 weekly | median 21 months | DMFS | Experimental – mean 10.5; Control – mean 8 | Experimental – mean 14.4; Control – mean 14.3 | None reported |
| 2/day brush and 1/day rinse | Debonding | WSL index | Experimental – mean 1.02 SD 0.08; Control – mean 1.0 SD 0.02 | Experimental – mean 1.05 SD 0.13; Control – mean 1.08 SD 0.17 | None reported |
| 6 weekly | Debonding | DMFS | Experimental – mean 2.8 SD 4.2; Control – mean 2.7 SD 3.8 | Experimental – mean 7.62; Control – mean 19.34 | None reported |
| 2 monthly | Debonding | WSL index | Experimental – mean 0.31 SD 1.07; Control – mean 0.43 SD 1.68 | Experimental – mean 1.02 SD 3.00; Control – mean 4.79 SD 5.58 | No side effects occurred |
| 2 monthly | 6-8 months | WSL index | Experimental – 0; Control – 0 | Experimental – 37.5%; Control – 32.3% | None reported |
| 2/day | Debonding (Mean 1.8 yrs SD 0.53) | WSL index | Experimental – mean 0.3 SD 1.0; Control – mean 1.0 SD 1.8 | Experimental – mean 0.4 SD 1.0; Control – mean 1.2 SD 1.8 | None reported |
| Daily practice | mean 24.5 months | DMFS and ICDAS | Experimental – 0; Control – 0 | Experimental – 30.6%; Control – 46.7% | None reported |
| Daily practice | 12 months | WSL index | [No of pts] Experimental – 4; Control – 5 | [No of pts] Experimental – 7; Control – 16 | None reported |
| 2/day F paste use; MI Varnish 3 monthly; MI Paste Plus 1/day; NaF rinse 1/day | 12 months | Enamel Decalcification Index and ICDAS | Experimental – mean 21.9 SD 1.3; Control – mean 21.1 SD 1.3 | Experimental – mean 22.3 SD 1.4; Control – mean 22.5 SD 1.5 | None reported |
Following the RoB assessment, three RCTs were included in the quantitative analysis, since the rest were heterogeneous and at high RoB. 25,27,31 Included studies had a total of 433 patients (10–20 years of age), of which 216 participants were allocated to the intervention group.
The eighteen RCTs were assessed for RoB (Table I). Ten studies were determined to have a high RoB and were excluded from the quantitative synthesis. 22,23,26,28,30,33,34,35,38,39 This led to the consideration of eight RCTs for meta-analysis. 24,25,27,29,31,32,36,37
Risk of bias assessment of RCTs included in the qualitative analysis.
| Trial | Bias from randomisation process | Bias from deviations from intended interventions | Bias from missing outcome data | Bias from measurement of the outcome | Bias from selection of the reported result | Overall bias |
|---|---|---|---|---|---|---|
| Ogaard et al. (1997) | High | Low | Low | Some concerns | Low | High |
| Alexander et al. (2000) | High | Some concerns | Low | Some concerns | Low | High |
| Jenatschke et al. (2001) | Some concerns | Low | Low | Some concerns | Some concerns | Some concerns |
| Weiss et al. (2005) | Some concerns | Some concerns | Low | High | Some concerns | High |
| Ogaard et al. (2006) | Some concerns | Low | Low | Low | Low | Some concerns |
| Steckson-Blicks et al. (2007) | Some concerns | Low | Low | Low | Some concerns | Some concerns |
| Al Mulla et al. (2010) | Some concerns | Low | Low | High | Some concerns | High |
| Jiang et al. (2013) | Low | Low | Low | Low | Some concerns | Some concerns |
| Fretty (2014) | Low | Low | Low | High | Some concerns | High |
| Sonesson et al. (2014) | Low | Some concerns | Low | Low | Some concerns | Some concerns |
| Hoffman et al. (2015) | Some concerns | Low | High | High | Some concerns | High |
| Suetenkov et al. (2015) | Some concerns | Some concerns | Low | High | Some concerns | High |
| van der Kaaij et al. (2015) | Low | Low | Low | Low | Some concerns | Some concerns |
| Esenlik et al. (2016) | High | Some concerns | High | High | Some concerns | High |
| Zotti et al. (2016) | Low | Low | Low | Low | Some concerns | Some concerns |
| Alavi et al. (2018) | Some concerns | Some concerns | High | High | Some concerns | High |
| Gómez et al. (2018) | High | Low | Some concerns | Low | Some concerns | High |
| Rechmann et al. (2018) | Low | Some concerns | Low | Low | Low | Some concerns |
Of the eight trials considered for quantitative synthesis, five evaluated the same intervention – topical F application. 24,25,27,29,31 The five RCTs identified a reduction in WSL development. The other trials investigated chlorhexidine, oral hygiene, and CPP-ACP. 32,36,37 A slight reduction in WSL incidence was obtained by these interventions, which was reported as non-significant. The studies could not be pooled for meta-analysis, since they were heterogeneous interventions.
Of the five F intervention RCTs, three used placebo controls. 25,27,31 The other two RCTs used F in their intervention and comparison arms. 24,29 One RCT compared a toothpaste combining SnF2 and AmF to a NaF toothpaste with the same F concentration. 24 While another compared two toothpastes of different F concentration. 29 Since these studies prevented the estimation of effect size, it was decided to synthesise data from the three trials that compared the effects of F to a placebo. 25,27,31
Two studies compared the effect of professionally applied F. 25,27 They investigated the effects of a six-weekly application of 0.9% difluorsilane (1000 ppm F) in a polyurethane varnish base and a two-monthly application of 12,300 ppm APF foam. 25,27 Conversely, the effect of daily at-home use of a 250 ppm NaF rinse was investigated using quantitative light induced fluorescence (QLF) by another trial. 31 Compliance with the use of a mouthrinse was not recorded. The F interventions were supplementary to standard oral hygiene practice of twice daily brushing with a fluoridated toothpaste.
In the three RCTs, a clinical assessment was performed under artificial white lighting following plaque removal. 25,27,31 Patients with developmental defects of enamel (DDE) such as hypoplasia and fluorosis were excluded in one study. 27 The other two RCTs did not consider DDE. 25,31 The diagnosis and assessment of WSLs differed between the studies. The teeth were dried with sterile gauze prior to clinical examination in one RCT. 27 Clinical photographs were taken after drying the teeth in two RCTs. 25,31 The bonding materials used to attach appliances varied between the RCTs. One study did not provide this information. 31 Resin composite was used in one trial, while the other study used a resin applied as a pre-coated bracket (Victory Twin APC II bracket, 3M Unitek, CA, USA). 25,27 All three RCTs had some concerns related to RoB (Figure 2).
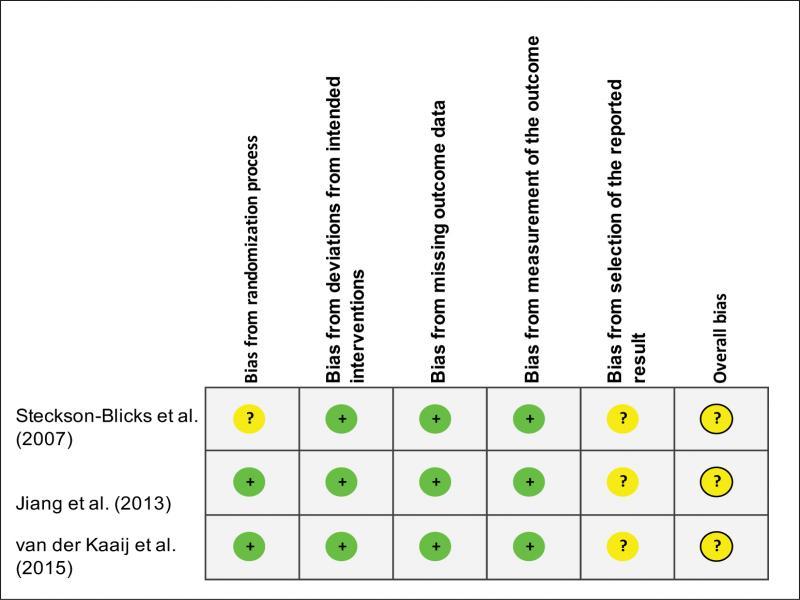
Risk of bias summary of studies included in the meta-analysis.
The pooled effect size from the random-effects model showed a risk difference of -0.23 (95% CI: -0.35, -0.11, p < 0.001; Figure 3). A 23% reduction in WSL incidence was obtained with F interventions. Similar results were obtained using a fixed-effects model (Supplementary Figure 1). Statistical heterogeneity was moderate at 49.3% (Figure 4). Only one study investigated the effect of F on lesion size. 31 Since there were no WSLs at the start of the study for these participants, the effect on lesion inhibition could not be ascertained.
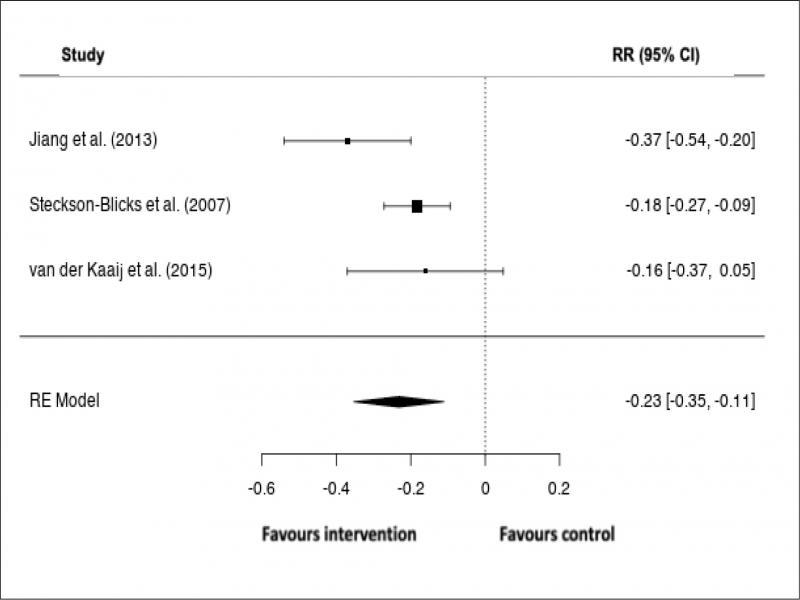
Meta-analysis of WSL risk reduction with fluoride interventions, using a random-effects model. The forest plot shows the pooled effect of fluoride on WSL incidence.
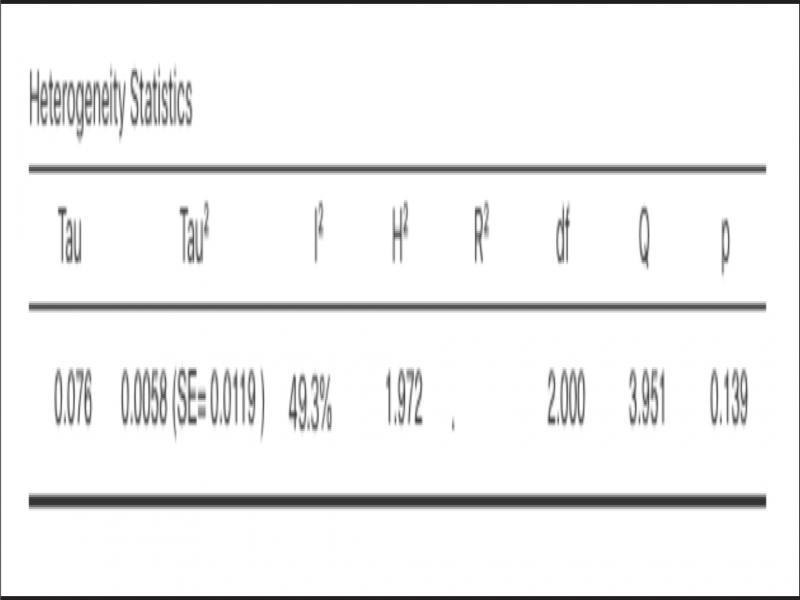
Heterogeneity assessment.
The publication and reporting biases were not analysed since fewer than ten studies were included in the meta-analysis. Subgroup analyses were not conducted due to insufficient data. A pooled adverse effect profile for F could not be constructed, since only one study reported adverse events, of which there were none. 27
The findings from the quantitative analysis of the three included RCTs were used for grading F interventions. 25,27,31 The quality of evidence for CHX, CPP-ACP, oral hygiene program and laser interventions were graded from the initial full-texts analysed. This included the RCTs and observational studies.
According to the GRADE evaluation, a moderate quality of evidence for the use of F during orthodontic care was obtained (Figure 5). Quality was downgraded to moderate due to statistical heterogeneity and a small number of RCTs. Very low-quality evidence was obtained for CHX, CPP-ACP, oral hygiene program and laser therapy, due to non-randomised studies that were sponsor funded and measured surrogate outcomes (Figure 5).
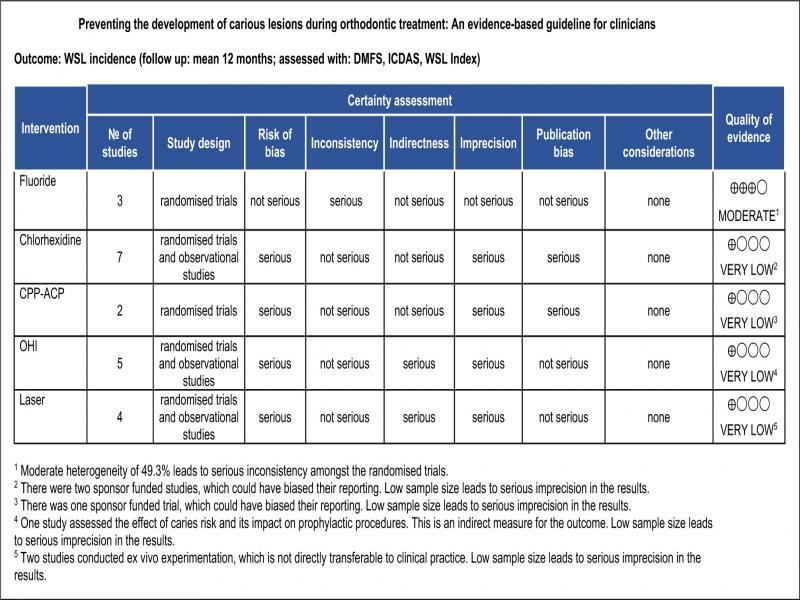
GRADE evidence profile: caries prevention during orthodontic treatment.
The primary resource to evaluate is the intervention, both in-chair and at-home. The cost of F interventions may vary within and across countries, and could be shared by governments, private insurers and patients. A cost-benefit analysis regarding F for caries prevention has not been conducted previously. Therefore, an economic evaluation could not be performed in the present review. Since these caries preventive resources are not labour intensive, a resource use evaluation may not be important in developing clinical recommendations.
For policy makers in governments, institutions and health insurers, the use of F during orthodontic treatment is recommended for adoption as a policy. For most healthy patients undergoing orthodontic treatment, the use of F as a caries preventive measure is advocated. For patients who prefer to avoid F, appropriate advice from the clinician is recommended. Clinicians are advised to routinely use topical F during orthodontic care.
In the present SR, the effect of interventions in the prevention of WSLs during orthodontic treatment was evaluated. Previous SRs have several limitations (Supplementary Table IV), including the inclusion of high-risk studies. These include in vitro, in vivo, ex vivo, retrospective, non-RCT and split mouth design studies (Supplementary Table V). It is critical to conduct sensitivity analyses to evaluate whether studies associated with a high risk of bias influence the pooled estimate. This aspect has been lacking in previous published SRs. Additionally, several SRs included studies that considered WSL inhibition post-orthodontic treatment. Since complete reversal is unachievable with current interventions, it is imperative to prevent WSLs. 40,41 This counters the undesirable aesthetic and biologic consequences of WSL development.
Previous systematic reviews and meta-analyses.
| Systematic reviews | |||||||
|---|---|---|---|---|---|---|---|
| Author | Pre-registered? | Intervention | Studies used | Risk of bias done? | GRADE? | Guideline? | Comments |
| Derks (2004) | N | F, CHX, GIC | RCTs and split mouth studies | N | N | N | Split mouth studies-clustering effect not considered (11/16 = 69% of included studies). Overall risk of bias not calculated. |
| Benson et al (2013) | Y | F | RCTs | Y | Y | N | Cochrane review |
| Lapenaite et al (2016) | N | F and CPP-ACP | RCTs and quasi-RCTs | N | N | N | No risk of bias assessment |
| Rahimi et al (2017) | N | F varnish | RCTs, in vitro and in vivo | N | N | N | in vitro, in vivo studies used |
| Imani et al (2019) | N | CPP-ACP | RCTs | Y | N | N | Post orthodontic WSL reduction. |
| Pithon et al (2019) | Y | CPP-ACP | RCTS and non-RCTs | Y | N | N | Non-RCTs used |
| Sardana et al (2019) | Y | Self applied F | RCTs and quasi-RCTs | Y | Y | N | During and post-orthodontic studies included without sub group analyses. Both control and intervention are F. |
| Meta-analyses | |||||||
|---|---|---|---|---|---|---|---|
| Author | Pre-registered? | Intervention | Studies used | Risk of bias done? | GRADE? | Guideline? | Comments |
| Okada et al (2016) | Y | CHX varnish | RCTs and split mouth studies | N | N | N | Split mouth studies-clustering effect not considered (3/6 = 50% of included studies). Overall risk of bias not calculated. |
| Sardana et al (2019) | Y | Professionally applied F | RCTs and quasi-RCTs | Y | N | N | Follow up period ranges widely from short to long term, without appropriate analysis. |
| Tasios et al (2019) | Y | F, OHI, GIC | RCTs, quasi-RCTs and split mouth studies | Y | Y | N | Split mouth studies – clustering effect not considered (15/21 = 71% of included studies). |
Reasons for exclusion of studies included by previous SRs.
| Authors | Title | Reason | Exclusion stage |
|---|---|---|---|
| Adiaens et al. (1990) | The use of ‘Fluor Protector®’, a fluoride varnish, as a caries prevention method under orthodontic molar bands. | In vitro | Title/abstract screen |
| Twetman et al. (1995) | Effect of an antibacterial varnish on mutans streptococci in plaque from enamel adjacent to orthodontic appliances | Surrogate outcome | Title/abstract screen |
| Madléna et al. (2000) | Effect of chlorhexidine varnish on bacterial levels in plaque and saliva during orthodontic treatment | Surrogate outcome | Title/abstract screen |
| Demito et al (2004) | The efficacy of a fluoride varnish in reducing enamel demineralization adjacent to orthodontic brackets: an in vitro study. | In vivo | Title/abstract screen |
| Skold-Larsson, K. et al. (2004) | Effect of topical applications of a chlorhexidine/thymol-containing varnish on fissure caries assessed by laser fluorescence | Non RCT | Title/abstract screen |
| Luther et al. (2005) | Fluoride releasing glass beads in orthodontic treatment to reduce decay: a randomized, controlled clinical trial. | Outcome not reported | Title/abstract screen |
| Vivaldi-Rodrigues et al. (2006) | The effectiveness of a fluoride varnish in preventing the development of white spot lesions | Split mouth + <6 months | Title/abstract screen |
| Farhadian N, et al (2008) | Effect of fluoride varnish on enamel demineralization around brackets: an in-vivo study | In vivo | Title/abstract screen |
| Bailey et al. (2009) | Regression of post-orthodontic lesions by a remineralizing cream | Post-orthodontic | Title/abstract screen |
| Beerens et al. (2010) | Effects of casein phosphopeptide amorphous calcium fluoride phosphate paste on white spot lesions and dental plaque after orthodontic treatment: a 3-month follow-up | < 6 months | Title/abstract screen |
| Baeshen et al. (2011) | Effect of fluoridated chewing sticks (Miswaks) on white spot lesions in postorthodontic patients | Post-orthodontic | Title/abstract screen |
| Brochner et al. (2011) | Treatment of post-orthodontic white spot lesions with casein phosphopeptide-stabilised amorphous calcium phosphate | Post-orthodontic | Title/abstract screen |
| Enaia et al. (2011) | White-spot lesions during multibracket appliance treatment: A challenge for clinical excellence. | Non RCT | Title/abstract screen |
| Richter et al. (2011) | Incidence of caries lesions among patients treated with comprehensive orthodontics | Retrospective | Title/abstract screen |
| Robertson et al. (2011) | MI Paste Plus to prevent demineralization in orthodontic patients: a prospective randomized controlled trial | < 6 months | Title/abstract screen |
| Shinaishin et al. (2011) | Efficacy of light-activated sealant on enamel demineralization in orthodontic patients: an atomic force microscope evaluation | Ex vivo | Title/abstract screen |
| Akin et al. (2012) | Can white spot lesions be treated effectively? | Post-orthodontic | Title/abstract screen |
| Du et al. (2012) | Randomized controlled trial on fluoride varnish application for treatment of white spot lesion after fixed orthodontic treatment | Post-orthodontic | Title/abstract screen |
| Jumanca et al. (2012) | Infiltration Therapy-an Alternative to Fluoride Varnish Application for Treatment of White Spot Lesion After Fixed Orthodontic Treatment. | Post-orthodontic | Title/abstract screen |
| Huang et al. (2013) | Effectiveness of MI Paste Plus and PreviDent fluoride varnish for treatment of white spot lesions: a randomized controlled trial | Post-orthodontic | Title/abstract screen |
| Baroni et al. (2014) | A SEM and non-contact surface white light profilometry in vivo study of the effect of a creme containing CPP-ACP and fluoride on young etched enamel | In vivo | Title/abstract screen |
| Restrepo et al. (2015) | Control of white spot lesion adjacent to orthodontic bracket with use of fluoride varnish or chlorhexidine gel | In vivo | Title/abstract screen |
| He et al. (2016) | Comparative assessment of fluoride varnish and fluoride film for remineralization of postorthodontic white spot lesions in adolescents and adults over a 6-month period: a single-center, randomized controlled clinical trial, | Post-orthodontic | Title/abstract screen |
| Restrepo et al. (2016) | Control of White Spot Lesions with Use of Fluoride Varnish or Chlorhexidine Gel During Orthodontic Treatment A Randomized Clinical Trial. | < 6 months | Title/abstract screen |
| Kirschneck et al. (2016) | Efficacy of fluoride varnish for preventing white spot lesions and gingivitis during orthodontic treatment with fixed appliances-a prospective randomized controlled trial | < 6 months | Title/abstract screen |
| Singh et al. (2016) | Effects of various remineralizing agents on the outcome of post-orthodontic white spot lesions (WSLs): a clinical trial | Post-orthodontic | Title/abstract screen |
| Turska-Szybka et al. (2016) | Randomised Clinical Trial on Resin Infiltration and Fluoride Varnish vs Fluoride Varnish Treatment Only of Smooth-surface Early Caries Lesions in Deciduous Teeth. | Non-orthodontic | Title/abstract screen |
| Bock et al. (2017) | Changes in white spot lesions following post-orthodontic weekly application of 1.25 per cent fluoride gel over 6 months-a randomized placebo-controlled clinical trial. Part I: photographic data evaluation | Post-orthodontic | Title/abstract screen |
| Bock et al. (2017) | Changes in white spot lesions following post-orthodontic weekly application of 1.25 per cent fluoride gel over 6 months-a randomized placebo-controlled clinical trial. Part II: clinical data evaluation | Post-orthodontic | Title/abstract screen |
| Ebrahimi et al. (2017) | The effects of three remineralizing agents on regression of white spot lesions in children: a two week, single-blind, randomized clinical trial | < 6 months | Title/abstract screen |
| Karabekiroglu et al. (2017) | Treatment of post-orthodontic white spot lesions with CPP-ACP paste: A three year follow up study | Post-orthodontic | Title/abstract screen |
| Beerens et al. (2018) | Long-term remineralizing effect of MI Paste Plus on regression of early caries after orthodontic fixed appliance treatment: a 12-month follow-up randomized controlled trial | Post-orthodontic | Title/abstract screen |
| Heravi et al. (2018) | Effectiveness of MI Paste Plus and Remin Pro on remineralization and color improvement of postorthodontic white spot lesions | Post-orthodontic | Title/abstract screen |
The present review addressed these limitations through a rigorous approach. An a priori registration on the PROSPERO database, extensive search on multiple databases, and an independent analysis approach provided robustness in this review. The use of an updated Cochrane RoB 2 was also advantageous, since it identified an overall risk within the studies, and was less subjective compared to previous versions.
Eight studies were excluded due to their short duration of less than six months. A longer time frame was a key eligibility criterion because a short follow-up period is likely to be insufficient for clinically detectable signs of dental caries to develop in many individuals. Even when carious lesions are detected early, prior to cavitation, the demineralisation process may have been present for months or years. 2 The lack of adequate follow-up could lead to a type I error due to under-reporting of WSLs. Furthermore, several studies were excluded because they failed to include the presence of carious lesions (WSLs) as an outcome, and instead, resorted to report changes in microbiome, plaque and saliva. While these studies provided valuable insights into the mechanisms by which preventive measures reduce the risk of developing carious lesions, they cannot be considered equivalent to measuring the actual outcome of identifying WSLs. A reduction in certain cariogenic pathogens may not have an effect on WSL incidence, since the remineralisation-demineralisation balance is influenced by other factors. 2 These surrogate measures cannot yet be utilised as accurate markers of clinical disease.
The three RCTs included in the quantitative analysis investigated different F concentrations, and none were considered a low RoB. Two studies in the meta-analysis did not have an initially calculated sample size. 25,31 One RCT calculated the sample size required as 132 participants per group. 25 Following attrition, this became 132 and 125 per group. Similarly, another RCT required 47 participants per group following their power calculation. 31 Subsequent to dropouts, the groups were 36 and 45. These discrepancies could affect the statistical power of the studies, due to the risk of a type II error. One study had no pre-specified analysis plan, which created a potential for bias in the analysis post hoc. 27 Although the outcome measures differed between the three RCTs as the analysis was based on the proportion of WSL incidence, this did not affect the synthesis. The heterogeneity obtained could be explained by the differing concentration and delivery vehicles of F in these trials. Since the number of studies assessed was low, heterogeneity analysis might be misleading due to decreased sensitivity.
The GRADE evaluation considers the number and design of studies in addition to effect sizes, which highlighted the lack of RCTs on the topic. The recommendation to use F during orthodontic treatment supports the current widespread usage by dental professionals. 42 F therapy could include professional delivery as part of clinical care, or at-home use of F rinses and toothpastes. However, reported poor compliance with mouth rinsing by orthodontic patients reduces the clinical effectiveness of at-home therapies. 43 Since F interventions alone provide a 23% risk reduction of WSL development during orthodontic care, the combination of other preventive measures could reduce the risk further. Proper oral hygiene and non-cariogenic dietary practices in combination with F interventions may be of greater importance to reduce the risk of WSL incidence. The present review was unable to evaluate the cost-effectiveness of interventions, as no appropriate studies were identified, an important consideration that is likely to favour at-home therapy. No RCTs were conducted to investigate the preventive effects of self-assembling peptides (SAP), RMGIC coatings and other calcium products such as TCPs. The meta-analysis was planned to be performed using Stata, but Jamovi statistical software was used, due to its open and free access.
There are several limitations associated with this review. The World Health Organization International Clinical Trials Registry Platform was not sought for unpublished studies, which could have provided additional relevant papers. The exclusion of non-English papers may have omitted well-conducted relevant studies. Since only three RCTs were pooled for meta-analysis, the estimates of risk difference may differ from the results obtained. Nevertheless, both random and fixed effects models provided similar outcomes. The results related to the inhibition of WSL progression and patient reported outcomes were not investigated in the included studies.
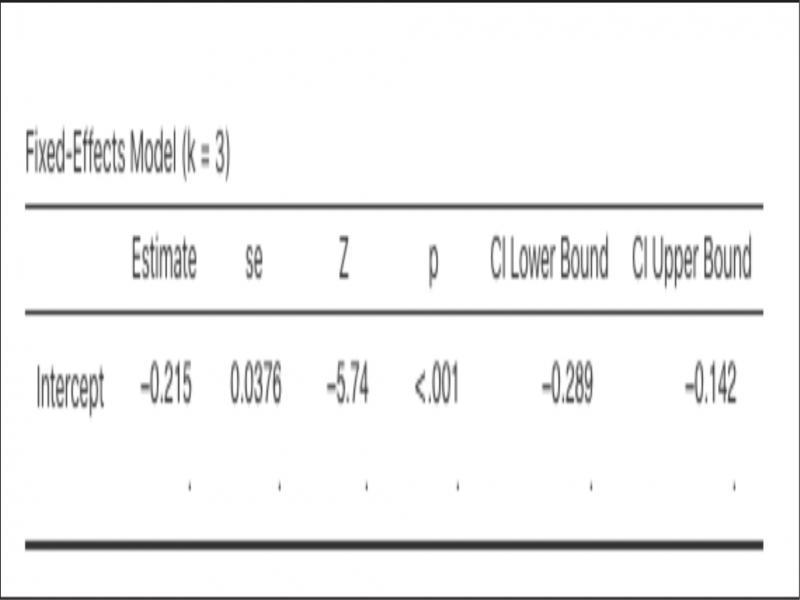
Pooled risk difference obtained from a fixed-effects model.
Future RCTs should explore the efficacy of interventions such as SAP, RMGIC, CPP-ACP and TCP on the prevention of WSLs during orthodontic treatment. Authors are encouraged to report on caries increment/lesion transition and adverse effects. Prospective RCTs should register their study protocols a priori and have a follow-up period of the duration of care, or otherwise at least six months. Future investigators are encouraged to design trials for patients undergoing removable orthodontic treatment.
-
Based on the results of this SR, the use of supplementary fluoride is recommended for carious lesion prevention during fixed appliance orthodontic treatment.
-
Only low-quality evidence supports the use of CHX, CPP-ACP, OHI and lasers for caries prevention during orthodontic care.
-
Fluoride-based preventive interventions provide a 23% risk reduction of WSL incidence during fixed appliance orthodontic treatment.
-
Additional well-conducted RCTs are required to provide caries preventive recommendations during fixed and removable appliance orthodontic treatment.
-
The investigation of newer interventions is required to update this clinical guideline.