
Soon after the discovery of activating mutations of epidermal growth factor receptor (EGFR) and of their crucial role in determining sensitivity to tyrosine kinase inhibitors (TKIs), several trials confirmed the advantage of TKIs in comparison to chemotherapy for patients with advanced non-small cell lung cancer (NSCLC) with activating EGFR mutations.1-5 Due to higher response rate, longer time to progression and less toxicity, monotherapy with TKIs has been approved as the preferred first-line treatment for these patients. TKIs clearly improve short-term prognosis of patients with EGFR mutant lung cancer. Still, after a median interval of around one year, patients on treatment with TKIs develop resistance and experience disease progression.6 New treatments, either as first-line or at progression are needed.7
After huge disappointment due to four large negative trials of chemotherapy alone versus chemotherapy combined with continuous application of gefitinib or erlotinib8-11, the idea of combining TKIs with chemotherapy never fully recovered. Many research groups simply concluded that the two categories of drugs should not be used together and most of current pre-clinical and clinical research focuses on new drugs designed to overcome primary or acquired resistance to TKIs.12-14 The fact that the four trials were unselected regarding histology and smoking status received little attention. For a quarter of patients in the TRIBUTE trial, the status of EGFR mutations was later determined: when treated with the combination in comparison to chemotherapy alone, EGFR mutant patients had higher response rate and a trend towards longer progression-free survival (PFS), but no advantage in overall survival (OS).15
In spite of prevailing disappointment, some researchers insisted that the negative message of the four large trials should be accepted as new knowledge rather than ignored and developed the concept of intercalated treatment. The reasoning was clear: when applied concomitantly with chemotherapy, TKIs induce G1-phase cell-cycle arrest, due to which cell-cycle dependent chemotherapeutic agents will not be effective.16 Chemo-refractoriness of cells harboring sensitizing-EGFR mutations in the presence of gefitinib was confirmed in vitro.17 Time separation with an interval of 6 days without TKIs to restore chemosensitivity of tumor cells should remove this mutual antagonism, so as to benefit from the efficacy of both classes of drugs.18 Additional support for the concept of intercalated treatment came from laboratory experiments and from a clinical trial of sequential application of chemotherapy and TKI: proper sequence starting with cytotoxic drugs, followed by TKIs leads to their synergistic activity.19-23
So far, a few dozen clinical trials on intercalated treatment with chemotherapy and TKIs have been published. A recent review focused on trials with randomization between intercalated schedules and chemotherapy alone.24 While such a review is definitively valuable, a reader is confused when facing a list of trials with a wide range of eligibility criteria, leading to diverging conclusions. This review paper has a different goal. We believe that before proceeding with further clinical research, we should understand which patients will most likely benefit from intercalated treatment. Only after defining the optimal target p opulation, future trials can be designed to compare intercalated treatment to the best standard treatment in those selected patients.
Published papers and conference r eports on intercalated therapy for NSCLC were eligible for review. Intercalated treatment was defined as a treatment with cytotoxic drug(s), combined with an EGFR-TKI during a part of a treatment cycle. Trials on chemotherapy combined with continuous application of TKIs or a gap of less than 4 days, and trials using alternating cycles of cytotoxic drugs and of TKIs were not included in this review.
Pubmed was used to search for published trials on intercalated treatment for NSCLC, with the following descriptors and limits: NSCLC; chemotherapy and (erlotinib and/or gefitinib and/ or afatinib); clinical trial; 2006-2016 as the publication period; humans; English language. This initial search led to 686 publications. The list was then manually reviewed. Additional publications were identified using Web of Science cross-citation database, proceedings of major conferences during the past 4 years (IASLC World Lung Cancer Conference, ASCO, ESMO, European Lung Cancer Conference) and the list of references in published trials.
Selected papers were analyzed, with focus on selection criteria and parameters of efficacy. Information on the proportion of patients with EGFR mutant tumors was often incomplete or missing. If not available in the text, an estimate on the proportion of patients with EGFR mutant disease was made. As the first step, all patients with squamous histology were considered as EGFR wild-type (EGFR wt). In case of non-squamous histology, an estimate was based on proportion of never-smokers vs. smokers and on ethnicity, using published meta-analysis on global pattern of EGFR mutations.25
Due to the wide spectrum of eligibility criteria and of comparator arms, randomized trials were not considered an appropriate basis for analysis of efficacy of the intercalated treatment. We therefore chose a different approach. Experience from single-arm phase II trials and from the intercalated arm of randomized trials was analyzed in relation to histology, smoking status and EGFR mutation status, separately for treatment-naive and pre-treated patients. Median PFS was taken as a conventional indicator of efficacy.
Statistical analysis was limited to intercalated treatment, either in non-randomised trials or in the intercalated arm of randomised trials. The strength of correlation between proportion of non-squamous tumors, proportion of non-smokers and proportion of EGFR-mutation positive cases with median PFS was evaluated calculating the Pearson’s correlation coefficient (R) and the coefficient of determination (R-squared; R2). Pearson’s R is a simple measure of the linear correlation between two variables, giving a value between +1 and -1, where +1 is a total positive correlation, 0 is the absence of correlation, and -1 is a total negative correlation. The coefficient of determination is such that 0 ≤ R2 ≤ 1: although there are no specific cut-offs to define a moderate, or a strong correlation, a higher R2 score indicates a stronger association.
Correlations were graphically described by bubble plots, where each bubble represents a study, with bubble size proportional to the number of patients included in each study. As all the analyses were weighted by sample size of each study, weighted least-squares regression line was calculated and reported in each graph.
Statistical analyses were conducted using SPlus (S-PLUS 6.0 Professional, release 1; Insightful Corporation, Seattle, WA, USA). Graphs were realized using SigmaPlot (Systat Software, San Jose, CA).
After the initial search through PubMed, 96 reports were selected to which 4 trials found through conference proceedings and 6 trials identified by cross-citation database were added for a total of 106 studies. A total of 29 trials were considered eligible for the analysis (Figure 1). The series includes 11 single-arm phase II trials, 16 randomized phase II trials and 2 phase III randomized trials, with a total of 2903 patients.26-54
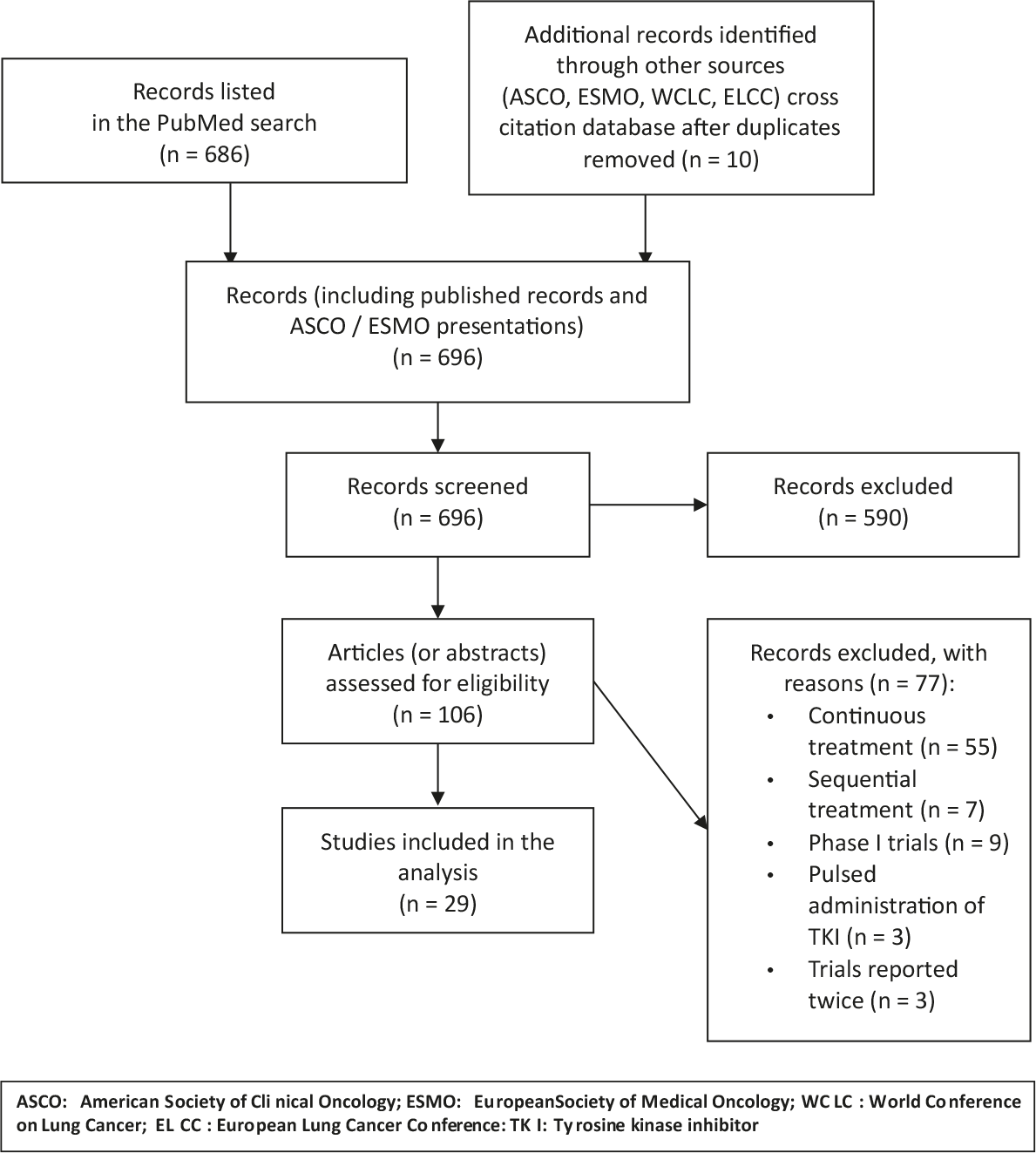
Flow diagram on selection of publications for analysis.
Fourteen trials were limited to non-squamous histology, while 15 included patients with any histologic type of NSCLC. Sixteen trials were open only for treatment-naive patients, while 13 included those in progression after first-line treatment. The proportion of never-smokers was specified in all but two reports.
Five trials were limited to EGFR mutant disease and 4 to patients with EGFR wild-type or unknown tumors. Another 3 trials included a substantial proportion of EGFR mutant cases and separately reported the experience for this subpopulation of patients. Nine of the remaining 17 trials included information on EGFR status for some of their patients, but the proportion analyzed was usually low and thus inappropriate for any analysis.
Erlotinib and gefitinib were used in 17 and 9 trials, respectively. In 2 trials, either erlotinib or gefitinib was used, while afatinib was used in 1 trial.
Among 18 randomized trials (Table 1), chemotherapy alone was the comparator arm in 10 trials. Four trials used TKI alone as the comparator, 2 trials compared two different intercalated schedules, while 2 trials used 3-arm design with comparison among intercalated schedule, chemotherapy alone or TKIs alone. According to PFS as the most common parameter of efficacy, the intercalated schedule was superior to the comparator in 12 trials, crossing the conventional margin of P < 0.05 in 7 trials. No significant difference was seen in 4 other trials and in 2 trials comparing two different intercalated schedules of intercalated therapy.
Randomized trials on intercalated chemotherapy and TKIs for non-small cell lung cancer
| REFERENCE | TYPE OF TRIAL | # OF PTS | SELECTION OF PATIENTS | TREATMENT REGIMEN(s) | % never-smokers | % EGFR mutant, intercalated arm only | ORR (%) | MEDIAN PFS (months) | MEDIAN OS (months) |
|---|---|---|---|---|---|---|---|---|---|
| Mok 2009 | Randomized | 154 | All histologies, | Arm A (76 pts): | 34% | 28% | Arm A: 35.5% | Arm A: 6.9 m | Arm A: 17.3 m |
| (FASTACT) 26 | Phase 2 | previously untreated | Gem, d 1 & 8 | Arm B: 24.4% | Arm B: 5.5 m | Arm B: 17.7 m | |||
| Cis or Carbo, day 1 | |||||||||
| Erlotinib, d 15-28 | P = 0.12 | P = 0.002 | P: ns | ||||||
| Cycle q 4 weeks | |||||||||
| Arm B (78 pts): | |||||||||
| as above, placebo | |||||||||
| instead of Erlotinib | |||||||||
| 52 | As above, | Arm A (24 pts) | 100% | 49% | Arm A: 45.8% | Arm A: 11.1 m | Not reached | ||
| neversmokers | Arm B (28 pts) | Arm B: 32.1% | Arm B: 6.4 m | ||||||
| Treatment as above | P: not | P = 0.002 | |||||||
| reported | |||||||||
| Hirsch 2011 27 | Randomized | 143 | Positive for EGFR | Arm A (71 pts): | 28% | 10% | Arm A: 22.4% | Arm A: 4.6 m | Arm A: 11.4 m |
| Aerts 2012 | Randomized | 231 | All histologies | Arm A (115 pts): | 7% | 4% | Arm A: 7% | Arm A: 4.9 m | Arm A: 5.5 m |
| Lee 2013 29 | Randomized | 240 | Non-squamous, | Arm A (78 pts): | 100% | 56% | Arm A: 44.7% | Arm A: 7.4 m | Arm A: 20.5 m |
| Wu Y-L 2013 | Randomized | 451 | All histologies, | Arm A (226 pts): | 49% | 39% | Arm A: 44% | Arm A: 7.6 m | Arm A: 18.3 m |
| 97 | As above, subgroup | Arm A (49 pts): | Not | 100% | Arm A: 84% | Arm A: 16.8 m | Arm A: 31.4 m | ||
| Auliac 2014 31 | Randomised | 147 | EGFR wild-type or | Arm A (73 pts): | 7.5% | 4% | Arm A: 4.4% | Arm A: 2.2 m | Arm A: 6.5 m |
| Karavasilis | Randomized | 50 | All histologies | Arm A (25 pts): | 10% | 11% | Arm A: 24% | Arm A: 2.9 m | Arm A: 9.9 m |
| Mok 2014 33 | Randomized | 123 | Unselected, | Arm A (63 pts): | 24% | 28% | Arm A: 13% | Arm A: 3.5 m | Arm A: 7.6 m |
| Yu 2014 34 | Randomized | 117 | Non-squamous, | Arm A (58 pts): | 58% | 40% | Arm A: 50.0% | Arm A: 7.9 m | Arm A: 25.4 |
| 32 | As above, subgroup | Arm A: 14 pts | Not | 100% | Arm A: 76.9% | Arm A: | Not reached | ||
| Choi 2015 35 | Randomized | 90 | NSCLC, EGFR wild. | Arm A (44 pts): | 10% | 10% | Arm A: 41.9% | Arm A: 4.1 m | Arm A: 9.3 m |
| Juan 2015 36 | Randomized | 68 | All histologies | Arm A (33 pts): | 6% | 5% | Arm A: 3% | Arm A: 3.0 m | Arm A: 7.5 m |
| Lu 2015 37 | Randomized | 219 | Adenocarcinoma, | Arm A (109 pts): | 100% | 72% | Not reported | Arm A: 10 m | Not reported |
| Michael | Randomized | 54 | All histologies | Arm A (28 pts): | 15% | 12% | Arm A: 6% | Arm A: 2.5 m | Arm A: 3.9 m |
| Han 2016 39 | Randomized | 121 | Adenocarcinoma, | Arm A (40 pts): | Not | 100% | Arm A: 82.5% | Arm A: 18.8 m | Not reached |
| Lara 2016 | Randomized | 59 | PS 2, Proteomics: | Arm A (33 pts): | 20% | 20% | Arm A: 6% | Arm A: 1.6 m | Arm A: 6.0 m |
| Li 2016 41 | Randomized | 79 | Predominantly non- | Arm A (27 pts): | Not | 19% | Arm A: 10% | Arm A: 2.9 m | Arm A: 8.3 m |
| Lee 2016 42 | Randomized | 76 | Adenocarcinoma, | Arm A (39 pts): | 100% | 42% | Arm A: 79.5% | Arm A: 12.8 m | Arm A: 29.2 m |
| 29 | As above, EGFR | Arm A: 15 pts | 100% | 100 | Arm A: 86.7% | Arm A: 13.3 m | Arm A: 26.6 m | ||
| 37 | As above, | Arm A: 22 pts | 100% | 0 | Arm A: 72.7% | Arm A: 6.6 m | Arm A: 29.2 m | ||
| Yoon 201643 | Randomized | 87 | Non-squamous | Arm A (57 pts): | 31% | 31% | Arm A: 31.8 % | Arm A: 5.7 m | Arm A: 12.1 m |
Carbo = carboplatin; Cis = cisplatin; Doce = docetaxel; Gem = gemcitabine; ORR = overall response rate; OS = overall survival; Pacli = paclitaxel; PFS = progression-free survival; Pem = pemetrexed; PTS = patient
Basic data on single-arm Phase 2 trials are presented in Table 2.
Single-arm Phase II trials on intercalated chemotherapy and TKIs for non-small cell lung cancer
| REFERENCE | # OF PTS | SELECTION OF PATIENTS | TREATMENT REGIMEN(s) | % never-smokers | % EGFR mutant | ORR (%) | MEDIAN PFS (months) | MEDIAN OS (months) |
|---|---|---|---|---|---|---|---|---|
| Oshita 2010 44 | 16 | Unselected, | Pacli d 1 | Not reported | 25% | 43.8% | Not reported | 18.1 m |
| Sangha 2011 45 | 39 | All histologies | Doce d 1 | 28% | 19% | 28.2% | 4.1 m | 18.2 m |
| Minami 2013 46 | 27 | Non-squamous | Pem, d 1 | 22% | 4% | 11.1% | 2.8 m | 15.8 m |
| Yoshimura 2013 47 | 27 | Activating EGFR | Pem, d 1 | 78% | 100% | 25.9% | 7.0 m | 11.4 m |
| Kim 2014 48 | 17 | Non-squamous, | Pem d 1 | 27% | 0% | 27.0% | 2.5 m | 6.7 m |
| Fang 2014 49 | 57 | Unselected, | Gem, d 1 and 8 | 37% | 40% | 11% | 10 m | 15.2 m |
| Yang 2014 50 | 29 | Adenocarcinoma, | Pacli, d1 | 100% | 73% | 74.1% | 16 m | Not reached |
| Zwitter 2014 51 | 15 | Adenocarcinoma, | Gem d 1 and 4 | 100% | 5% | 33% | 6.0 m | 7.6 m |
| Yoshimura 2015 52 | 26 | Activating EGFR | Pem d 1 | 46% | 100% | 84.6% | 18.0 m | 32.0 m |
| Yu 2015 53 | 42 | Mostly | Pem, d 1 or Pem + | 71% | 61% | 23.8% | 8.0 m | 11.0 m |
| Zwitter 2016 (ITAC 2) 54 | 38 | Activating EGFR | Gem d 1 and 4 | 63% | 100% | 84.2% | 23.4 m | 38.3 m |
Carbo = carboplatin; Cis = cisplatin; Doce = docetaxel; Gem = gemcitabine; Irino = irinotecan; ORR = overall response rate; OS = overall survival; Pacli = paclitaxel; PFS = progression-free survival; Pem = pemetrexed; PTS = patient
Figure 2 shows correlation between median PFS and proportion of patients with non-squamous histology (Panel A), proportion of never-smokers (Panel B) and proportion of EGFR mutant patients (Panel C).
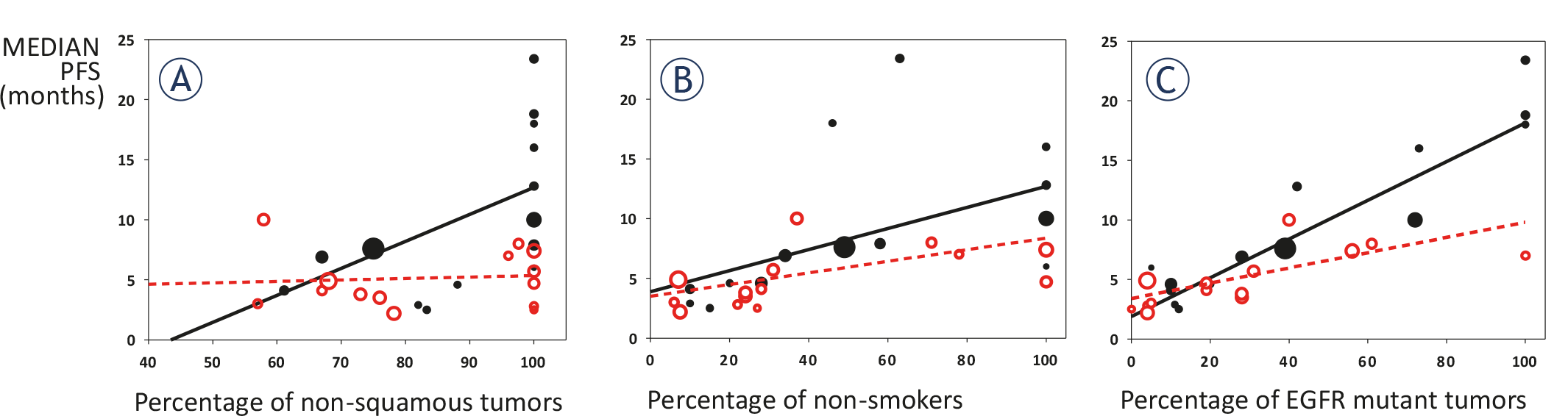
Correlation between median PFS and proportion of patients with non-squamous histology (A), proportion of never-smokers (B) and proportion of EGFR mutant patients (C). Black solid marks and black solid lines are for 1st line treatment; red hollow marks and red interrupted lines for 2nd line treatment. Bubble size corresponds to the number of patients in a trial.
As for tumor histology, there was a moderate correlation between proportion of non-squamous tumors and median PFS in the first-line setting (R = 0.61, R2 = 0.38, p = 0.02). The slope of the regression line (0.23) suggests that a 10% increase in the proportion of non-squamous tumors corresponds to a 2.3-months improvement in median PFS in first-line. On the other hand, the correlation was very weak in the second-line setting (R = 0.09, R2 = 0.01, p = 0.77).
As for smoking status, there was a moderate correlation between proportion of non-smokers and median PFS, both in the first-line and in the second-line setting (first-line: R = 0.55, R2 = 0.30, p = 0.04; second-line: R = 0.65, R2 = 0.42, p = 0.02). In detail, the slope of the regression line (0.09 for the first-line and 0.05 for the second-line) suggests that a 10% increase in the proportion of non-smokers corresponds to a 0.9-months improvement in median PFS in first-line, and to a 0.5-months improvement in median PFS in second-line.
As for EGFR mutational status, there was a strong correlation between proportion of EGFR mutation-positive tumors and median PFS, both in the first-line and in the second-line setting (first-line: R = 0.91, R2 = 0.83, p < 0.0001; second-line: R = 0.69, R2 = 0.48, p = 0.006). The slope of the regression line (0.16 for the first-line and 0.06 for the second-line) suggests that a 10% increase in the proportion of EGFR mutation-positive tumors corresponds to a 1.6-months improvement in median PFS in first-line, and to a 0.6-months improvement in median PFS in second-line.
Six trials on treatment-naive patients with EGFR mutant disease reported excellent response rate of 83.1% (range: 76.9% to 84.2%).30,34,39,42,52,54 Five of these trials presented data on median PFS ranging from 13.3 to 23.4 months (median PFS for all 5 trials: 18.6 months). This figure does not include an additional trial from this category which reported 86% PFS at 15 months, with no data on median PFS due to relatively short follow-up.34
Most surveys and meta-analyses focus on the question of efficacy and/or toxicity of a particular new treatment in comparison with the standard approach. This was also the case with intercalated treatment for advanced NSCLC. On the basis of published randomized trials, a recent meta-analysis concluded that intercalated treatment is superior to the comparator arm.24 While this meta-analysis offered a valuable insight into an area which is not in the main stream of current clinical research, the question of efficacy of intercalated treatment is too complex to be answered by a simple comparison.
A critical look at all published trials reveals great heterogeneity in eligibility criteria including treatment-naive patients or those in progression after first-line therapy. In addition, we see a whole spectrum of biologically divergent disease: all histologic types or only non-squamous histology; exclusively EGFR-mutant disease, only EGFR-wt tumors or, in most trials, both groups. On such a heterogeneous basis and without considering the optimal standard therapy for a particular population of patients, the value of a new approach cannot be assessed. Is the intercalated treatment superior to chemotherapy alone for EGFR-wt patients or superior to TKI alone for EGFR-mutant patients? To be more concrete: it comes as no surprise that intercalated treatment was superior to chemotherapy alone for a population which included a substantial proportion of EGFR-mutant patients;26,29, 30,34,37,39,42 and superior to TKIs alone for a population of predominantly EGFR-wt patients.36,40 It is not the intercalated approach, but inclusion of an effective drug into the schedule which may be responsible for the positive experience in these trials. We believe that on the basis of randomized clinical trials published so far, the question of superiority of intercalated schedules over the standard treatment cannot be answered.
Our estimate on the proportion of EGFR mutant patients, as used in the analysis, includes a considerable degree of uncertainty. Only half of trials (14/29) included information on the proportion of EGFR-mutant vs. EGFR-wt tumors for more than 50% of patients. Other trials reported results of EGFR analysis for a minority of patients, or (in 8 publications) no such information. We therefore made an estimate, based on histologic types of tumors (available for 28/29 trials), on proportion of never-smokers (available for 27/29 trials) and on the country where a trial was performed, using tables from a recent meta-analysis.25 This approach led us to the best possible estimate, but the results should nevertheless be regarded as exploratory and tentative. In future, precise molecular diagnostics should minimize these uncertainties.
Our survey does not include analysis of toxicity of different schedules of intercalated treatment. This aspect was clearly presented in a recent review: apart from the expected skin toxicity and diarrhea, intercalated schedules do not present a disproportional burden to patients.24
Relation between selection criteria and effectiveness of intercalated treatment is shown in Figure 2. On the basis of pooled data on median PFS from randomized and single-arm trials, it is clear that pre-treated patients are not good candidates for a treatment which includes a modality to which resistance has already developed. While the proportion of patients with non-squamous histology and of never-smokers determine efficacy of intercalated treatment, EGFR mutations are clearly the strongest predictive factor for longer PFS. By far the greatest benefit was for treatment-naive patients with activating EGFR mutations. According to trials in which this group of patients was reported separately, their median PFS after intercalated treatment ranged between 13.3 and 23.4 months; median PFS for the pooled data was 18.4 months. This figure is substantially above PFS of 9 to 13 months, as reported for TKIs as monotherapy for EGFR-mutant NSCLC.26,55-58 Response rate was also very high: 83.1%, with a substantial proportion of complete remissions. Our survey is in accordance with a recent editorial and with a meta-analysis, which pointed to intercalated regimens as the most promising first-line treatment for EGFR- mutated NSCLC.59,60
With the introduction of liquid biopsy from peripheral blood, the category of patients with undetermined EGFR mutant status should be very small.61 In case this new technique is not available, previously untreated never-smokers with non-squamous histology for whom EGFR status cannot be determined should also be considered for trials testing the role of intercalated treatment. Depending on ethnicity, approximately half of them have EGFR mutant tumors, in which case addition of TKI to cytotoxic drugs would be clearly beneficial; the other half with EGFR negative tumors should benefit from cytotoxic drugs included in the intercalated schedule.
In future trials of intercalated treatment, pemetrexed with platin appears as the preferred option for the cytotoxic component. Regarding the choice of TKI, virtually all current experience is limited to erlotinib and gefitinib. Still, in view of recent very favorable experience for patients who developed resistance mutations, osimertinib intercalated with chemotherapy deserves to be considered either in first-line setting or for patients in progression after first-generation TKIs.62
In two recent phase II randomized trials, patients with treatment-naive advanced EGFR- mutant NSCLC were treated with continuous gefitinib in combination with chemotherapy. As the comparator arm, sequential gefitinib and chemotherapy or gefitinib alone were applied.63, 64 In both trials, patients on the combination with continuous gefitinib and chemotherapy experienced longer PFS. These reports support the advantage of combined treatment with chemotherapy and TKIs and re-open the dilemma between their concomitant and intercalated application. Combination of TKIs with bevacizumab is another possibility which deserves further attention.65
We are perfectly aware that the correlation we have reported between the proportion of patients with EGFR mutation positive tumor and the median PFS obtained with the intercalated treatment could be reasonably observed also with EGFR inhibitors alone. The only way to assess the real added value of intercalated treatment is a randomized trial with comparison to TKI alone and overall survival as the principal endpoint.
In conclusion, intercalated treatment with cytotoxic drugs and TKIs is a promising approach for patients with previously untreated advanced NSCLC with activating EGFR mutations, as well as for never-smokers with adenocarcinoma and undetermined EGFR status. For these patients, randomized trials with comparison to the optimal standard treatment, or possibly to a third arm with continuous application of TKIs in combination with chemotherapy should define the preferred treatment approach.